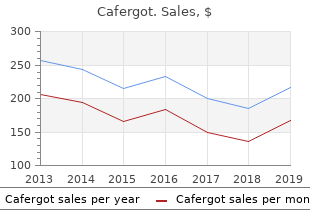
"Cheap cafergot 100 mg online, pain management treatment for spinal stenosis."
By: Cristina Gasparetto, MD
- Professor of Medicine
- Member of the Duke Cancer Institute

https://medicine.duke.edu/faculty/cristina-gasparetto-md
The cardinal features at presentation as well as during Cardiac manifestations occur in 11% initially and in the disease course are shown in Table 46-6 back pain after treatment for uti cheap generic cafergot canada. The cardiac and diarrhea are the two most common symptoms wrist pain treatment tendonitis cafergot 100 mg free shipping, disease is due to blue ridge pain treatment center harrisonburg va order cafergot overnight delivery fibrosis involving the endocardium pain & depression treatment effective 100mg cafergot, prioccurring in up to pain swallowing treatment discount 100mg cafergot fast delivery 73% initially and in up to florida pain treatment center order cafergot with a visa 89% durmarily on the right side, although left side lesions can ing the course of the disease. The dense fibrous deposits are most comof sudden onset; it is a deep red or violaceous erythema monly on the ventricular aspect of the tricuspid valve of the upper body, especially the neck and face, often and less commonly on the pulmonary valve cusps. They associated with a feeling of warmth, and occasionally can result in constriction of the valves, and pulmonic associated with pruritus, lacrimation, diarrhea, or facial stenosis is usually predominant, whereas the tricuspid edema. Flushes may be precipitated by stress, alcohol, valve is often fixed open, resulting in regurgitation preexercise, certain foods such as cheese, or by certain dominating. Up to 80% of patients with cardiac lesions agents such as catecholamines, pentagastrin, and serodevelop heart failure. Flushing episodes may be less extensive, occur in 30% at autopsy, and most frebrief, lasting 2�5 min, especially initially, or may last quently affect the mitral valve. Flushing is Other clinical manifestations include wheezing or usually seen with midgut carcinoids but can also occur asthma-like symptoms (8�18%) and pellagra-like skin with foregut carcinoids. A variety of noncardiac problems due fiushes are frequently prolonged for hours to days, redto increased fibrous tissue have been reported including dish in color, and associated with salivation, lacrimation, retroperitoneal fibrosis causing urethral obstruction, diaphoresis, diarrhea, and hypotension. The fiush associPeyronie�s disease of the penis, intraabdominal fibrosis, ated with gastric carcinoids is also reddish but patchy in and occlusion of the mesenteric arteries or veins. Pathobiology Diarrhea is present in 32�73% initially and 68�84% at some time in their disease course. Diarrhea usually In different studies, carcinoid syndrome occurred in 8% occurs with fiushing (85% of cases). The diarrhea is usuof 8876 patients with carcinoid tumors with a rate of ally described as watery with 60% having <1 L/day of 1. It only occurs when sufficient concentrations of secreted products by the tumor reach the systemic circulation. All carSymptoms/signs cinoid tumors do not have the same propensity to Diarrhea 32�73% 68�84% metastasize and cause the carcinoid syndrome. Midgut Flushing 23�65% 63�74% carcinoids account for 60�67% of the cases of carcinoid Pain 10% 34% syndrome, foregut tumors for 2�33%, hindgut for 1�8%, Asthma/wheezing 4�8% 3�18% and an unknown primary location for 2�15% (Tables Pellagra 2% 5% 46-2, 46-3). Up to Male 46�59% 46�61% 50% of dietary tryptophan can be used in this synthetic Age pathway by tumor cells, which can result in inadequate Mean 57 yrs 52�54 yrs supplies for conversion to niacin; hence some patients Range 25�79 yrs 9�91 yrs (2. Foregut carcinoids are the most likely to cause to histamine release because it can be prevented by H1 an atypical carcinoid syndrome. Numerous studies show One of the most immediate life-threatening complitachykinins are stored in carcinoid tumors and released cations of the carcinoid syndrome is the development during fiushing. The crises P, suggesting that other mediators must be involved in may occur spontaneously or be provoked by stress, the fiushing. Patients develop ble for the wheezing as well as the fibrotic reactions intense flushing, diarrhea, abdominal pain, and cardiac involving the heart, causing Peyronie�s disease and abnormalities including tachycardia, hypertension, or intraabdominal fibrosis. Metaboment of urinary or plasma serotonin or its metabolites in lites of fenfiuramine, as well as the dopamine receptor the urine. False-positive elevations may occur if the tion of which is known to cause fibroblast mitogenesis. Studies on cultured interstitial cells from is taking certain medications (cough syrup containing human cardiac valves demonstrate that these valvuloguaifenesin, acetaminophen, salicylates, or L-dopa). In one study, 92% of patients with carcinoid growth factor and collagen biosynthesis. Both the magnitude of serotonin tion rate; however, plasma and platelet serotonin levels, if overproduction and prior chemotherapy are important available, may give additional information. Because patients with foregut patients with cardiac disease, but its role in the pathocarcinoids may produce an atypical carcinoid syndrome, genesis is unknown. Patients with mild to moderate symptoms Ketanserin diminishes diarrhea in 30�100% of patients. A escape control after a median of 4 months, and the dose combination of histamine H1 and H2 receptor antagonists may need to be increased. In patients with carcinoid crises, somatostatin anaSynthetic analogues of somatostatin (octreotide, lanlogues are effective at both treating the condition as reotide) are the most widely used agents to control the well as preventing symptoms during known precipitatsymptoms of patients with carcinoid syndrome (Fig. This includes a right hemimg/month) gives a plasma level 1 ng/mL for 25 days, colectomy for appendiceal carcinoid, an abdominoperwhereas this requires 3�6 injections per day of the nonineal resection or low anterior resection for rectal sustained-release form. Each of the sustained-release forms is highly in diameter,a simple appendectomy is proposed by some effective at controlling the symptoms of the carcinoid for appendiceal tumors, whereas others favor a formal syndrome (61�85% of patients). For 1to 2-cm rectal carcinoids, a Short-term side effects occur in 40�60% of patients wide local full-thickness excision is performed. Important long-term side effects include gallrecommend antrectomy in type 1 to reduce the hyperstone formation, steatorrhea, and deterioration in gastrinemia; antrectomy produced regression of the glucose tolerance. Hepatic course of the disease does the tumor per se cause promiartery embolization can have major side effects includnent symptoms such as abdominal pain. Because 15�69% of small-intestinal carcisecretion usually causes the presenting symptoms and noids this size have metastases, some recommend a wide can cause life-threatening complications. More than 98% the tumors except insulinomas, >50% are malignant of patients with gastrinomas have fasting hypergastrine(Table 46-2); therefore, treatment must also be directed mia, although in 40�60% the level may be less than tenagainst the tumor itself. Therefore, when the diagnosis is suspected, quently widespread, surgical resection for cure, which a fasting gastrin level should be determined first. If the gastrin level is elevated, it is imporhypergastrinemia causes gastric acid hypersecretion tant to show it is increased when gastric pH 2. In patients with hypergasunusual locations, most patients have a typical duodenal trinemia with fasting gastrin <1000 ng/L and gastric ulcer. In patients with gastrinomas without ases), or without Helicobacter pylori present. Chronic unexplained stimulation test is usually positive, with the criterion of diarrhea should also suggest gastrinoma. Gastric acid hypersecretion in patients with gastrinomas Most gastrinomas (50�70%) are present in the duodecan be controlled in almost every case by oral gastric num, followed by the pancreas (20�40%) and other antisecretory drugs. Because of their long duration of intraabdominal sites (mesentery, lymph nodes, biliary action and potency, allowing once or twice a day dostract, liver, stomach, ovary). Three cases with two extraabing, the proton pump inhibitors are the drugs of choice. About 60�90% of gastrinomas roidism increases the sensitivity to gastric antisecretory are malignant (Table 46-2) with metastatic spread to drugs and decreases the basal acid output. Distant metastases to bone occur With the increased ability to control acid hypersecrein 12�30% of patients with liver metastases. At presenDiagnosis tation careful imaging studies are essential to localize the extent of the tumor. A third of patients present with the diagnosis of gastrinoma requires the demonstration hepatic metastases, and in <15% of those with hepatic of fasting hypergastrinemia and an increased basal gastric insulin levels should decrease to <43 pmol/L (<6 �U/mL) 591 metastases the disease is limited, so that surgical resecwhen blood glucose decreases to 2. Surgical cure is possible in 30% of (40 mg/dL) and the ratio of insulin to glucose is <0. Therefore, all patients with gasserum proinsulin level, an insulin/glucose ratio >0. The increased use of these specific patients have symptoms due to excess catecholamine insulin assays has resulted in increased numbers of release secondary to the hypoglycemia including sweatpatients with insulinomas having lower plasma insulin ing, tremor, and palpitations. Characteristically these values than the 43 pmol/L (6 �U/mL) levels proposed to attacks are associated with fasting. In these patients Insulinomas are generally small (>90% < 2 cm), usuthe assessment of proinsulin and C-peptide levels at the ally not multiple (90%), and only 5�15% are malignant; time of hypoglycemia are particularly helpful for estabthey almost invariably occur only in the pancreas, dislishing the correct diagnosis. In different studies, 75�95% of patients are insulinomas, in addition to elevated plasma insulin levels, cured by surgery. Before surgery, the hypoglycemia can elevated plasma proinsulin levels are found and Cbe controlled by frequent small meals and the use of peptide levels can be elevated. Diazoxide is a benzothiadiazide whose hyperglycemic effect is attributed to inhibiDiagnosis tion of insulin release. Approxithe diagnosis of insulinoma requires the demonstration mately 50�60% of patients respond to diazoxide. Other of an elevated plasma insulin level at the time of hypoagents effective in some patients to control the hypoglycemia. A number of other conditions may cause glycemia include verapamil and diphenylhydantoin. However, liver disease, alcoholism, poor nutrition, or other extraoctreotide needs to be used with care because it inhibits pancreatic tumors. The most reliable test to diagnose growth hormone secretion and can alter plasma glucagon insulinoma is a fast up to 72 h with serum glucose, Clevels; therefore, in some patients it can worsen the peptide, and insulin measurements every 4�8 h. If they are not effective, various anti-tumor treatjust cited obtained before glucose is given. Some 70�80% ments such as hepatic arterial embolization, chemoemof patients develop hypoglycemia during the first 24 h bolization, or chemotherapy have been used (see later). There is no general distinction in the literature between a tumor that A glucagonoma is an endocrine tumor of the pancreas contains somatostatin-like immunoreactivity (somatothat secretes excessive amounts of glucagon, which causes statinoma) and does (11�45%), or does not (55�89%) a distinct syndrome characterized by dermatitis, glucose produce a clinical syndrome (somatostatinoma synintolerance or diabetes, and weight loss. The cases of somatostatinomas, only 11% were associated tumor is clinically heralded by a characteristic dermatitis with the somatostatinoma syndrome. The mean age of (migratory necrolytic erythema) (67�90%), accompanied patients is 51 years. Somatostatinomas occur primarily in by glucose intolerance (40�90%), weight loss (66�96%), the pancreas and small intestine, and the frequency of the anemia (33�85%), diarrhea (15�29%), and thromboemsymptoms differs in each. The rash starts usually as an annular more frequent in pancreatic than intestinal somatostatinerythema at intertriginous and periorificial sites, espeomas: diabetes mellitus (95% vs 21%), gallbladder disease cially in the groin or buttock. It subsequently becomes (94% vs 43%), diarrhea (92% vs 38%), steatorrhea (83% raised and bullae form; when the bullae rupture, eroded vs 12%), hypochlorhydria (86% vs 12%), and weight loss areas form. Somatostatinomas occur in the pancreas in tic laboratory finding is hypoaminoacidemia, which 56�74% of cases, with the primary location in the panoccurs in 26�100% of patients. The tumors are usually solitary (90%) and Glucagonomas are generally large tumors (5�10 cm) large, with a mean size of 4. From 50�82% have evidence of metastatic spread at preSomatostatin is a tetradecapeptide that is widely dissentation, usually to the liver. It is a potent inhibitor of many Diagnosis processes including release of almost all hormones, acid secretion, intestinal and pancreatic secretion, and intestithe diagnosis is confirmed by demonstrating an nal absorption. Most of the clinical manifestations are increased plasma glucagon level (normal is <150 ng/L). Plasma glucagon levels are >1000 ng/L in 90%, between 500 and 1000 ng/L in 7%, and <500 ng/L in 3%. A Diagnosis plasma glucagon level >1000 ng/L is considered diagnostic of glucagonoma. Other diseases causing increased plasma In most cases somatostatinomas have been found by glucagon levels include renal insufficiency, acute pancreaccident either at the time of cholecystectomy or during atitis, hypercorticism, hepatic insufficiency, prolonged endoscopy. Duodetion of cirrhosis, these disorders do not increase plasma nal somatostatin-containing tumors are increasingly glucagon to >500 ng/L. The diagnosis of the somatostatinoma syndrome requires the demonstration of elevated plasma somatostatin levels. Long-acting presentation,whereas 30�69% of small-intestinal somatosomatostatin analogues such as octreotide or lanreotide statinomas have metastases. Surgery is the treatment of improve the skin rash in 75% of patients and may choice for those without widespread hepatic metastases. The mean age of patients with logues such as octreotide or lanreotide are the drugs of this syndrome is 49 years; however, it can occur in chilchoice. In nonresponsive patients the combination of glucocorthe principal symptoms are large-volume diarrhea ticoids and octreotide has proved helpful in a small (100%) severe enough to cause hypokalemia (80�100%), number of patients. Other drugs reported to be helpful dehydration (83%), hypochlorhydria (54�76%), and in small numbers of patients include prednisone flushing (20%). The diarrhea is secretory in nature, (60�100 mg/d), clonidine, indomethacin, phenothpersisting during fasting, is almost always >1 L/d and iazines, loperamide, lidamidine, lithium, propranolol, and >3 L/d in 70%. Treatment of advanced disease with ing steatorrhea (16%), and the increased stool volume is embolization, chemoembolization, and chemotherapy due to increased excretion of sodium and potassium, may also be helpful (see later). In children <10 years old, the syndrome is and hepatic metastases (64�92%), and the tumors are usually due to ganglioneuromas or ganglioblastomas and usually large (72% >5 cm). By fasting the patient, a (30�80%); jaundice (20�35%); weight loss, fatigue, or number of causes can be excluded that cause marked diarbleeding; and 10�15% are found incidentally. Other diseases that can give a secretory large-volume age time from the beginning of symptoms to diagnosis diarrhea include gastrinomas, chronic laxative abuse, carciis 5 years. The diagnosis is established by histologic confirmation in a patient without either clinical symptoms or elevated plasma hormone levels. These should strongly suggest the diagnosis in a patient with a patients may require 5 L/d of fiuid and >350 meq/day of pancreatic mass because it is usually normal in patients potassium. The tumors are usually large, and liver ure, old age, infiammatory conditions, and diabetes. The proposal that this could be a discrete synUnfortunately, surgical curative resection can be considdrome is supported by finding that 25�42% of patients ered only in the minority of the patients because with medullary thyroid cancer with hypercalcitonemia 64�92% present with metastatic disease. Patients have a mean age of 38 years, and the symptoms are usually due to either Localization of the primary tumor and defining the acromegaly or the tumor itself. Surgery is the treatment of choice somatostatin receptors (sst1�5), radiolabeled octreotide if diffuse metastases are not present. Long-acting somatobinds with high affinity to sst2 and sst5, lower for sst3, statin analogues such as octreotide or lanreotide are the and has a very low affinity for sst1 and sst4. However, this method gives only regional localization and therefore is reserved for cases where other imaging modalities are negative. For patients with foregut carcinoids without hepatic metastases, the 5-year survival in one study was 95% and with distant 100 No liver metastases (n = 158) 90 80 p < 0. A number of different modalities are reported 177lutetium-coupled analogues, which emit both and to be effective in advanced disease including cytoreduc-rays. These results suggest this novel therapy may be helpful, especially in patients with advanced metastatic disease.
Dysfibrinogenemia A hereditary condition in which there is a structural alteration in the fibrinogen molecule pain management in dogs and cats discount 100 mg cafergot free shipping. Dyshematopoiesis Abnormal formation and/or development of blood cells within the bone marrow sacroiliac joint pain treatment exercises buy on line cafergot. Dyspoiesis Abnormal development of blood cells frequently characterized by asynchrony in nuclear to chronic pain treatment center venice fl order cafergot cheap cytoplasmic maturation and/or abnormal granule development unifour pain treatment center statesville buy cafergot cheap online. Echinocyte A spiculated erythrocyte with short joint pain treatment in homeopathy purchase cafergot 100 mg line, equally spaced projections over the entire outer surface of the cell pain spine treatment center darby pa buy cafergot master card. Effector lymphocytes Antigen stimulated lymphocytes that mediate the efferent arm of the immune response. The cell is an oval to elongated ellipsoid with a central area of pallor and hemoglobin at both ends; also known as ovalocyte, pencil cell, or cigar cell. Embolism the blockage of an artery by embolus, usually by a portion of blood clot but can be other foreign matter, resulting in obstruction of blood flow to the tissues. Embolus A piece of blood clot or other foreign matter that circulates in the blood stream and usually becomes lodged in a small vessel obstructing blood flow. Endothelial cells Flat cells that line the cavities of the blood and lymphatic vessels, heart, and other related body cavities. Granules contain acid phosphatase, glycuronidase cathepsins, ribonuclease, arylsulfatase, peroxidase, phospholipids, and basic proteins. Eosinophilia An increase in the concentration of eosinophils in the peripheral blood (>0. Associated with parasitic infection, allergic conditions, hypersensitivity reactions, cancer, and chronic inflammatory states. Erythroblastic island A composite of erythroid cells in the bone marrow that surrounds a central macrophage. These groups of cells are usually disrupted when the bone marrow smears are made but may be found in erythroid hyperplasia. The least mature cells are closest to the center of the island and the more mature cells on the periphery. It is caused by an antigen� antibody reaction in the newborn when maternal antibodies traverse the placenta and attach to antigens on the fetal cells. It contains the respiratory pigment hemoglobin, which readily combines with oxygen to form oxyhemoglobin. The cell develops from the pluripotential stem cell in the bone marrow under the influence of the hematopoietic growth factor, erythropoietin, and is released to the peripheral blood as a reticulocyte. The average life span is about 120 days, after which the cell is removed by cells in the mononuclear-phagocyte system. Erythrocytosis An abnormal increase in the number of circulating erythrocytes as measured by the erythrocyte count, hemoglobin, or hematocrit. Erythrophagocytosis Phagocytosis of an erythrocyte by a histiocyte; the erythrocyte can be seen within the cytoplasm of the histiocyte as a pink globule or, if digested, as a clear vacuole on stained bone marrow or peripheral blood smears. Erythropoiesis Formation and maturation of erythrocytes in the bone marrow; it is under the influence of the hematopoietic growth factor, erythropoietin. Essential A myeloproliferative disorder affecting primarily thrombocythemia the megakaryocytic element in the bone marrow. Also called primary thrombocythemia, hemorrhagic thrombocythemia, and megakaryocytic leukemia. Evan�s syndrome A condition characterized by a warm autoimmune hemolytic anemia and concurrent severe thrombocytopenia. Extracellular matrix Noncellular components of the hematopoietic microenvironment in the bone marrow. Extramedullary Red blood cell production occurring outside the erythropoiesis bone marrow. Extramedullary the formation and development of blood cells at hematopoiesis a site other than the bone marrow. Extrinsic pathway One of the three interacting pathways in the coagulation cascade. The term extrinsic is used because the pathway requires a factor extrinsic to blood, tissue factor. This indicates a true pathologic state in the anatomic region, usually either infection or tumor. Faggot cell A cell in which there is a large collection of Auer rods and/or phi bodies. The result falling outside the control limits or violating a Westgard rule is due to the inherent imprecision of the test method. Small amounts can be found in the peripheral blood proportional to that found in the bone marrow. The presence of fibrin degradation products is indicative of either fibrinolysis or fibrinogenolysis. Fibrin monomer the structure resulting when thrombin cleaves the A and B fibrinopeptides from the and chains of fibrinogen. Fibrinogen group A group of coagulation factors that are consumed during the formation of fibrin and therefore absent from serum. The bonds between glutamine and lysine residues are formed between terminal domains of chains and polar appendages of chains of neighboring residues. The red tinge is caused by the presence of a glycoprotein and the purple by ribosomes. Flow chamber the specimen handling area of a flow cytometer where cells are forced into single file and directed in front of the laser beam. Fluorochrome Molecules that are excited by light of one wavelength and emit light of a different wavelength. Forward light scatter Laser light scattered in a forward direction in a flow cytometer. During normal lymphocyte development, rearrangement of the immunoglobulin genes and the T cell receptor genes results in new gene sequences that encode the antibody and surface antigen receptor proteins necessary for immune function. In humans, the genome consists of 3 billion base pairs of dna divided among 46 chromosomes, including 22 pairs of autosomes numbered 1�22 and the two sex chromosomes. Genotype the genetic constitution of an individual, often referring to a particular gene locus. It dehydrogenates glucose-6-phosphate to form 6phosphogluconate in the hexose monophosphate shunt. This provides the erythrocyte with reducing power, protecting the cell from oxidant injury. Glutathione A tripeptide that takes up and gives off hydrogen and prevents oxidant damage to the hemoglobin molecule. Glycoprotein Ib A glycoprotein of the platelet surface that contains the receptor for von Willebrand factor and is critical for initial adhesion of platelets to collagen after an injury. Glycosylated Hemoglobin that has glucose irreversibly hemoglobin attached to the terminal amino acid of the beta chains. Gower hemoglobin An embryonic hemoglobin detectable in the yolk sac for up to eight weeks gestation. Usually seen in bacterial infections, inflammation, metabolic intoxication, drug intoxication, and tissue necrosis. Granulomatous A distinctive pattern of chronic reaction in which the predominant cell type is an activated macrophage with epithelial-like (epithelioid) appearance. Gray platelet syndrome A rare hereditary platelet disorder characterized by the lack of alpha granules. Hairy cell the neoplastic cell of hairy cell leukemia characterized by circumferential, cytoplasmic, hairlike projections. Heinz bodies An inclusion in the erythrocyte composed of denatured or precipitated hemoglobin. Helmet cell Abnormally shaped erythrocyte with one or several notches and projections on either end that look like horns. Hematocrit the packed cell volume of erythrocytes in a given volume of blood following centrifugation of the blood. Expressed as a percentage of total blood volume or as liter of erythrocytes per liter of blood (L/L). Hematoma A localized collection of blood under the skin or in other organs caused by a break in the wall of a blood vessel. Hematopoiesis the production and development of blood cells normally occurring in the bone marrow under the influence of hematopoietic growth factors. Hematopoietic Specialized, localized environment in microenvironment hematopoietic organs that supports the development of hematopoietic cells. Hematopoietic stem cell Hematopoietic precursor cell capable of giving rise to all lineages of blood cells. Heme the nonprotein portion of hemoglobin and myoglobin that contains iron nestled in a hydrophobic pocket of a porphyrin ring (ferroprotoporphyrin). Hemoconcentration Refers to the increased concentration of blood components due to loss of plasma from the blood. Hemoglobin An intracellular erythrocyte protein that is responsible for the transport of oxygen and carbon dioxide between the lungs and body tissues. Hemoglobin distribution A measure of the distribution of hemoglobin width within an erythrocyte population. It is derived from the hemoglobin histogram generated by the Bayer/Technicon instruments. Hemoglobin Method of identifying hemoglobins based on electrophoresis differences in their electrical charges. Hemoglobinopathy Disease that results from an inherited abnormality of the structure or synthesis of the globin portion of the hemoglobin molecule. In hemolytic anemia this term refers to the premature destruction of erythrocytes. Hemolytic anemia A disorder characterized by a decreased erythrocyte concentration due to premature destruction of the erythrocyte. Hemolytic transfusion Interaction of foreign (nonself) erythrocyte reaction antigens and plasma antibodies due to the transfusion of blood. There are two types of transfusion reactions: immediate (within 24 hours) or delayed (occurring 2 to 14 days after transfusion). Hemopexin A plasma glycoprotein (globulin) that binds the heme molecule in plasma in the absence of haptoglobin. Hemosiderin A water insoluble, heterogeneous iron�protein complex found primarily in the cytoplasm of cells (normoblasts and histocytes in the bone marrow, liver, and spleen); the major long-term storage form of iron. Readily visible microscopically in unstained tissue specimens as irregular aggregates of golden yellow to brown granules. Hemosiderinuria Presence of iron (hemosiderin) in the urine; result of intravascular hemolysis and disintegration of renal tubular cells. Hemostasis the localized, controlled process that results in arrest of bleeding after an injury. Heparin A polysaccharide that inhibits coagulation of blood by preventing thrombin from cleaving fibrinogen to form fibrin. Commercially available in the form of a sodium salt for therapeutic use as an anticoagulant. The abnormal shape is due to a horizontal interaction defect with abnormal spectrin, deficiency or defect in band 4. Hereditary spherocytosisA chronic hemolytic anemia caused by an inherited erythrocyte membrane disorder. The vertical interaction defect is most commonly due to a combined spectrin and ankyrin deficiency. Secondary to membrane loss, the cells become spherocytes and are prematurely destroyed in the spleen. Hereditary A rare hemolytic anemia inherited in an stomatocytosis autosomal dominant fashion. The erythrocyte becomes dehydrated and appears as either target or spiculated cells. Hexose-monophosphate A metabolic pathway that converts glucose-6shunt phosphate to pentose phosphate. Histogram A graphical representation of the number of cells within a defined parameter such as size. Hodgkin lymphoma Malignancy that most often arises in lymph (disease) nodes and is characterized by the presence of Reed-Sternberg cells and variants with a background of varying numbers of benign lymphocytes, plasma cells, histiocytes, and eosinophils. Homologous Consists of two morphologically identical chromosomes that have identical gene loci, but may have different gene alleles as one member of a homologous pair is of maternal origin and the other is of paternal origin. On Romanowsky stained blood smears, it appears as a dark purple spherical granule usually near the periphery of the cell. Hydrops fetalis A genetically determined hemolytic disease (thalassemia) resulting in production of an abnormal hemoglobin (hemoglobin Bart�s, fi4) that is unable to carry oxygen. Hypercoagulable state A condition associated with an imbalance between clot promoting and clot inhibiting factors. Hypereosinophilic A term used to describe a persistent blood syndrome eosinophilia over 1. This can be brought about by an increase in the number of cells replicating, by an increase in the rate of replication, or by prolonged survival of cells. The stimulus for the proliferation may be acute injury, chronic irritation, or prolonged, increased hormonal stimulation; in hematology, a hyperplastic bone marrow is one in which the proportion of hematopoietic cells to fat cells is increased. Hypocellularity Decreased cellularity of hematopoietic precursors in the bone marrow. Hypochromic A lack of color; used to describe erythrocytes with an enlarged area of pallor due to a decrease in the cell�s hemoglobin content. Hypofibrinogenemia A condition in which there is an abnormally low fibrinogen level in the peripheral blood.
The cysts resemble comedones and the face pain solutions treatment center woodstock ga purchase cafergot with paypal, pinnae pain treatment center franklin tn purchase 100 mg cafergot overnight delivery, and dorsum are multifocally histologically are characterized by dilated follicles dilated and contain abundant arthropods (mites) 1 joint and pain treatment center lompoc ca order cafergot pills in toronto,5 plugged with abundant mites and keratin debris pain research treatment journal buy 100 mg cafergot otc. The microns in diameter with a chitinous exoskeleton pain medication for dogs metacam generic cafergot 100mg with visa, presence of mites in hair follicles of the pinnae pain treatment center lexington generic cafergot 100 mg on-line, as multiple jointed appendages, skeletal muscle, and was seen in this case, is a less common a reproductive tract containing basophilic 1 presentation. Similar mites are embedded in sides of the pinna and may need to be hyperkeratotic surface epithelium. There are 1 differentiated from notoedric ear mange, in multifocal 40 60 micron diameter basophilic which the lesion tends to be more superficial and eggs. Rare sections contain subcutaneous proliferative with mites embedded in the stratum inflammation characterized by lymphocytes, 4 corneum. Haired skin, mouse: There are numerous cross sections of follicles containing abundant keratin debris (comedones) (black arrows) arthropod parasites (mites) lining the wall of the comedone. External ear canal, mouse: There is a focal area of epidermal chitinous exoskeleton, obvious jointed appendages, and striated muscle. We receive few wild mice at contact1 and gravid females enter the hair follicles our laboratory but in our experience P. Pinna: Otitis externa, h y p e r k e r a t o t i c a n d lymphohistiocytic, diffuse, moderate, with infundibular adult mites and eggs. Conference Comment: For an institution with thousands of animals comprising hundreds of different species, this case serves as a reminder of the importance in monitoring the health of wildlife pests in addition to exhibit animal population. Psorergates simplex mites were once prevalent in laboratory mice but are now only readily recognized among wild and 4-5. Hair follicles, mouse: Centrally within the comedones, there are moderate numbers of yeasts and pet mice. Nidification of a mite participants discussed the finding of some (Psorergates simplex Tyrell, 1883: Myobiidae) in sections of mites which appeared to be larger the skin of mice. New for the fauna of Several species of mites are relatively common in Poland species of Psorergates spp. Upon histochemical staining, we are unable to determine the specific species of this fungus though we do not believe this morphology is consistent with Malassezia sp. The lack of inflammation associated with the dilated follicles was curious, as neither the mites nor fungi seemed to elicit a response from the host. In some slides, sections of ear pinna were identified which appeared to be the only area where lymphocytes and macrophages were recruited. We elected to include a third diagnosis for this location, though it is worth mentioning the mites seemed to be concentrated in larger numbers in these sections. Contributing Institution: Wildlife Disease Laboratories, Institute for Conservation Research, San Diego Zoo Global: Approximately 200 History: Chronic ascites; suspected neoplastic or ml of blood-tinged, watery fluid was present in inflammatory infiltrate in the liver. Histopathologic Description: Liver: the normal liver architecture is almost completely replaced Gross Pathologic Findings: the liver lobes by coalescing, variably dense aggregates of were diffusely enlarged, pale and rubbery, with a ductules and tubules separated by variably broad trabeculae of fibrous connective tissue in which are scattered capillaries. Ductules are lined by a single layer of cuboidal cells with light eosinophilic cytoplasm and central round to oval nuclei having uniformly granular chromatin, with 1-2 nucleoli. Golden-brown, granular pigment is present in the cytoplasm of some ductal epithelial cells, scattered macrophages and hepatocytes (hemosiderin). Scattered throughout the parenchyma are small foci of ducts with shrunken, hypereosinophilic cells, pyknotic nuclei and karyorrhectic debris (necrosis). Liver, iguana: the hepatic architecture is diffusely altered and replaced by a bright pink, hypocellular material. Cholangiocarcinomas can have a massive or m u l t i l o b u l a r appearance, are often u m b i l i c a t e d a n d protrude from the l i v e r c a p s u l. Pseudocarcinomatous biliary hyperplasia must also be differentiated from biliary hamartoma and cholangioma. In human and veterinary medicine, biliary hamartomas are rare and consist of ducts of varying caliber, unique cystic cavity f o r m a t i o n a n d 1-2. Liver, iguana: At higher magnification, hepatocytes are diffusely replaced by proliferating bile ducts separated 15,17 by a dense collagenous stroma. I n domestic animals, capsule are mildly to moderately thickened by cholangiomas are fibrous connective tissue. In L i v e r: S e v e r e, d i f f u s e, c h r o n i c, one retrospective study, 31% of all primary pseudocarcinomatous biliary hyperplasia with neoplasms in lizards affected the liver versus other organ systems,16 with malignant biliary marked interstitial fibrosis. Aflatoxins are excreted in the bile, two previously reported cases in female green causing periportal necrosis and inflammation in iguanas. With chronic exposure, there is bile biliary ductules replace the majority of normal duct hyperplasia and fibrosis, as described with chronic active hepatitis. Mild cellular atypia, the hyperplasia has been reported in an alpaca in absence of mitotic figures, and lack of invasion of association with parasitic ova of Fasciola hepatica,8,14 and hepatic coccidiosis. Liver, iguana: the collagenous stroma stains densely blue with Masson�s trichrome stain. These include granular receptor can be involved in epithelial hyperplasia, cell tumors,2 anaplastic large cell lymphoma,12 wound healing and tumorigenesis. The acini, clinical pathologic findings in this case to those which completely replace hepatic parenchyma in previously reported to assist in determining most sections, certainly appear to be biliary ducts whether the abdominal fluid is related to the and in our view, lack malignant characteristics as hepatic lesion. Oral granular cell variety of liver insults,5 many of which are tumors: An analysis of 10 new pediatric and mentioned by the contributor. Courville P, Wechsler J, Thomine E, Vergier differentiate into either biliary epithelium or B, Fonck Y, Souteyrand P, Beylot-Barry M, Bagot hepatocytes proliferate, as also may occur in M, Joly P, and the French Study Group On severe hepatic injury. Severe biliary fibrosis, which develops around hepatic venules, hyperplasia associated with liver fluke infection is termed periacinar fibrosis and occurs in an adult alpaca. Bile duct obstruction is not a prerequisite for type I biliary epithelial cell hyperplasia. Pseudocarcinomatous epithelial hyperplasia in the bladder unassociated with prior irradiation or chemotherapy. Solitary biliary hamartoma with cholelithiasis in a domestic rabbit (Oryctolagus cuniculus). Multiple biliary hamartomas: magnetic resonance features with histopathologic correlation. Analysis of the pathomorphology of the intraand extrahepatic biliary system in biliary atresia. In some sections of lung, Signalment: Southern hairy nosed wombat, alveoli are filled by hemorrhage and alveolar Lasiorhinus latifrons. History: Multiple free-ranging wild wombats Contributor�s Morphologic Diagnosis: 1). Lung: Multifocal alveolar hemorrhage and examination for a wombat health investigation congestion. Contributor�s Comment: Pulmonary Gross Pathology: adiaspiromycosis is caused by Emmonsia crescens or E. Moderate multifocal dorsal and lateral walled non-budding non-replicating adiaspores in alopecia with mild seborrhoea and tissue and elicit granulomatous inflammatory exudative dermatitis reactions in the host. Free the brushtail possum (Trichosurus vulpecula),9 within alveolar lumina or more commonly within most likely secondary to co-habitation of the multinucleated alveolar macrophages there are opossum with introduced British mammals (otter, many large spherical organisms (yeasts). Yeasts stoat, weasel, mole, red fox and pine martin) in measure 22 35 �m in diameter, have a thin 1-2 which E. Occasionally, subepithelial connective tissues of bronchioles are infiltrated by Wombats are large herbivorous burrowing aggregates of foamy macrophages forming small marsupials native to Australia, of which there are granulomas with intralesional yeasts. Lung, wombat: Alveoli contain moderate numbers of foamy macrophages and neutrophils with fewer multinucleated giant cell macrophage admixed with fibrin and cellular debris. Multinucleated macrophages range up to 70 �m and contained basophilic adiaspores with a 2-3 �m clear hyaline wall. The Aleuriospores of Emmonsia are ubiquitous and southern hairy nosed wombat is native to South soil borne, and on inhalation form thick-walled Australia and it is estimated that up to 100,000 non-replicating adiaspores in host tissues which remain in the wild. Infection of wombats case was culled and examined as part of a larger is thought to occur when they are pouch young, study examining skin disease and poor body and a linear increase in Emmonsia spherule size condition in wombats in the Murrayland region of with increasing wombat age has been observed. Pulmonary adiaspiromycosis was the habitat and burrowing habits of the wombat observed in all wild wombats culled concurrently is thought to render them prone to infections. Gross lung lesions were not evident Southern hairy nosed wombats spend up to threeat post mortem. Previously reported gross quarters of their time underground, and have findings in affected wombats have ranged from small home ranges centered around their clay/ minimal change, to pale consolidation of ventral calcrete or calcrete warrens. Adiaspiromycosis due to Emmonsia crescens is widespread in native Conference Comment: this is a unique look at British mammals. Burrow use and largely confined to the interstitium as adequately ranging behaviour of the southern hairy-nosed described by the contributor. Additionally, it was wombat (Lasiorhinus latifrons) in the not clear whether there was hemorrhage and Murraylands, South Australia. In: Australian Society of Veterinary Contributing Institution: School of Animal and Pathology Annual Meeting. Numerous eosinophilic, round, variable-sized (2-10 �m) Signalment: Male boa constrictor imperator, Boa intracytoplasmic inclusion bodies are present in constrictor imperator. Complete blood cell count In the kidney, almost all glomeruli show abundant revealed severe leukocytosis. These findings collagen deposition within the mesangium raised the suspicion for septicemia and, due to (glomerulosclerosis). Numerous intensely eosinophilic and tightly packed 2-�m granules are Gross Pathology: the animal was in poor body present in nephrocytes of the distal convoluted condition and showed severe cachexia. Numerous tubules (sexual segment) whereas epithelium of petechiae were present on ventral scales. The the proximal convoluted tubules contain coarsely coelomic cavity contained about 15 mL of clear granular brownish pigments (see discussion). Contributor�s Morphologic Diagnosis: Laboratory Results: Antemortem blood cell Kidney: count revealed severe leukocytosis with lymphocytosis (results not provided). Cytologic 1) Numerous intracytoplasmic eosinophilic analysis was performed on coelomic effusion and inclusions within renal tubular epithelium, revealed the presence of numerous bluish, consistent with inclusions of Inclusion Body homogenous, intracytoplasmic inclusions within Disease. Kidney, boa: Renal tubular epithelial cells contain one or more erythrocytes (arrowhead) contain homogenous bluish intracytoplasmic round, variably-sized eosinophilic intracytoplasmic inclusions (arrows). Epididymis, boa: Epididymal lining epithelium contains one or round, variably-sized eosinophilic intracytoplasmic inclusions (arrows). The genus arenavirus3 eosinophilic inclusions within epididymal is the only genus of the Arenaviridae family and epithelium, consistent with inclusions of Inclusion comprises 25 species according to the Body Disease. Two major lineages of arenaviruses eosinophilic inclusions with neurons and are described based on genetic differences and chromaffin cells, consistent with inclusions of geographical distribution: Old World arenaviruses Inclusion Body Disease. The discovery of virus-like particles by an important cause of fatal infection in organ transmission electron microscopy in affected transplantations recipients and immunocompetent tissues raised the suspicion for a viral etiology. Kidney, boa: Cells of the �sexual segment� of the distal convoluted capsules are markedly dilated (glomerulocystic disease). In pythons, these inclusions are mostly contained variable-sized acidophilic granules and found in the neurons of the central nervous brownish pigments. They are present in the distal convoluted cells of the central nervous system, in esophageal tubules, referred to as the �sexual segment�. The tonsils (epithelium and lymphoid cells), content of the granules is extruded into the gastrointestinal and respiratory epithelia, urinary wastes and is believed to represent hepatocytes, pancreatic acinar cells and renal pheromones that are useful for sexual courtship tubular epithelium. Epithelial cells of renal demonstrated in erythrocytes, lymphocytes and tubules, ureter, and epididymis and neurons: heterophils. Kidney, tubular epithelium: inclusions is variable, with boas having more Intracytoplasmic apicomplexans, few. As discussed by the contributor, the observation of v i r a l p r o t e i n inclusions and brown pigment within the tubular epithelium was f u r t h e r complicated by the prominent acidophilic 3-7. Kidney, boa: Renal tubules contain rare intraepithelial structures resembling coccidian (arrow), including one granules common schizont). It i s w o r t h Conference Comment: this case generated a lot mentioning this snake was in its reproductive of discussion, largely on the source of the season at the time of necropsy as the granules are unspecified brown inclusions within renal prominent and sperm production is abundant. The discussed differentials included the presence of glomerulosclerosis is a common protein, iron, copper, hemoglobin, melanin or finding in older reptiles; and we chose to separate lipofuscin. Unfortunately the contributor�s stains its diagnosis as most did not feel it was related to and our additional stains did not aid in their the viral infection. Inclusion body disease in Boid Comparative Veterinary Histology with Clinical snakes. Isolation, identification, and characterization of novel arenaviruses, the etiological agents of boid inclusion body disease. There are multifocal crypt abscesses characterized by Signalment: Snowy owl of unknown age and attenuated epithelium and intraluminal gender, Bubo scandiacus. Contributor�s Morphologic Diagnosis: Small Histopathologic Description: Small intestine: intestine: Enteritis, severe, acute, necrotizing and Multifocally, the mucosa and submucosa are ulcerative, multifocal, with intranuclear replaced by large areas of coagulation necrosis eosinophilic inclusion bodies (Cowdry A type) characterized by loss of cellular detail, consistent with strigid herpesvirus-1 infection. Occasionally, the necrosis and the cause of hepatosplenitis infectiosa strigum, a inflammatory cells extend through the tunica disease that affects only owls with a yellow or muscularis and to the serosa with multifocal mild orange iris and was first described in 19367 and further classified in 1973. Liver and spleen, snowy owl: the spleen and liver contain numerous necrotic foci ranging up to 0. Intestine, snowy owl: There are multifocal areas of transmural lytic necrosis scattered randomly along the section. Necrotic areas may appear in the show depression, anorexia, conjunctivitis, oral pharynx and small intestine as well. Conference Comment: Herpesvirus infection in birds of prey is caused by a member of the subfamily Alphaherpesvirinae. Intestine, snowy owl: Degenerate enterocytes within the intestine herpesvirus-2 in sheep.
Special Considerations/Preparation Available in 5-mg vial as a lyophilized powder pain treatment mayo clinic buy cafergot online now. Title Phenylephrine (Ophthalmic) Dose 1 drop instilled in the eye at least 10 minutes prior to upper back pain treatment exercises buy cafergot without prescription funduscopic procedures pain after lletz treatment generic cafergot 100 mg otc. Uses 657 Micormedex NeoFax Essentials 2014 Induction of mydriasis for diagnostic and therapeutic ophthalmic procedures treatment for residual shingles pain cheap 100 mg cafergot visa. The use of 10% solutions has caused systemic hypertension and tachycardia in infants pain treatment peptic ulcer cafergot 100 mg overnight delivery. Black Box Warning the rate of intravenous phenytoin administration should not exceed 1 to pain medication for dogs teeth discount cafergot 100 mg online 3 mg/kg/min (or 50 mg per minute, whichever is slower) in pediatric patients because of the risk of severe hypotension and cardiac arrhythmias. Although the risk of cardiovascular toxicity increases with infusion rates above the recommended infusion rate, these events have also been reported at or below the recommended infusion rate. Reduction in rate of administration or discontinuation of dosing may be needed [1]. Pharmacology Hepatic metabolism capacity is limited; saturation may occur within therapeutic range. Propylene glycol content of the intravenous formulation has been associated with seizures and may potentiate the cardiovascular effects of phenytoin. Dose related adverse events include nystagmus (total level 15 to 25 mg/L) and ataxia and mental status changes (total level greater than 30 mg/L). Phenytoin interacts with carbamazepine, cimetidine, 659 Micormedex NeoFax Essentials 2014 corticosteroids, digoxin, furosemide, phenobarbital, and valproate [1] [3] [4]. Use with caution in infants and children with hyperbilirubinemia: bilirubin displaces phenytoin from protein-binding sites, resulting in increased serum free phenytoin concentration [5]. Follow serum concentration closely: therapeutic range is 6 to 15 mcg/mL in the first weeks, then 10 to 20 mcg/mL due to changes in protein binding. Special Considerations/Preparation Injectable solution available in a concentration of 50 mg/mL. Product Information: Dilantin(R) intravenous injection solution, phenytoin sodium intravenous injection solution. Careful cardiac monitoring is needed during and after administering intravenous phenytoin. Although the risk of 661 Micormedex NeoFax Essentials 2014 cardiovascular toxicity increases with infusion rates above the recommended infusion rate, these events have also been reported at or below the recommended infusion rate. Bilirubin displaces phenytoin from protein-binding sites, resulting in increased serum free phenytoin concentration [6] [7] [8] [5] [9]. Adverse Effects Extravasation causes tissue inflammation and necrosis due to high pH and osmolality. Long-term effects of phenytoin include gingival hyperplasia, coarsening of the facies, hirsutism, hyperglycemia, and hypoinsulinemia. Cutaneous side effects include maculopapular exanthema, drug-induced lupus, and pigmentary alterations. Phenytoin interacts with carbamazepine, cimetidine, corticosteroids, digoxin, furosemide, phenobarbital, and valproate [1] [3] [4]. Monitoring Monitor electrocardiogram, blood pressure, and respiratory function continuously during infusion, and for 15 minutes to 1 hour after infusion [1] [2]. Special Considerations/Preparation 662 Micormedex NeoFax Essentials 2014 Injectable solution available in a concentration of 50 mg/mL. Amikacin, cefepime, ceftazidime, chloramphenicol, clindamycin, dobutamine, enalaprilat, fentanyl, heparin, hyaluronidase, hydrocortisone succinate, insulin, lidocaine, linezolid, methadone, micafungin, morphine, nitroglycerin, pentobarbital, potassium chloride, procainamide, propofol, sodium bicarbonate, and vitamin K1. Battino D: Clinical pharmacokinetics of antiepileptic drugs in paediatric patients. Phenytoin, carbamazepine, sulthiame, lamotrigine, vigabatrin, oxcarbazepine and felbamate. Reconstitute 2-g vial with 10 mL of sterile water for injection to make a final concentration of 200 mg/mL. Reconstituted solution stable for 24 hours at room temperature, 2 days refrigerated. Acyclovir, aminophylline, aztreonam, clindamycin, enalaprilat, esmolol, famotidine, heparin, hydrocortisone succinate, linezolid, lorazepam, magnesium sulfate, midazolam, milrinone, morphine, nicardipine, potassium chloride, propofol, ranitidine, remifentanil, and zidovudine. References Kacet N, Roussel-Delvallez M, Gremillet C, et al: Pharmacokinetic study of piperacillin in newborns relating to gestational and postnatal age. Pharmacology Piperacillin is a potent, broad-spectrum, semi-synthetic, ureidopenicillin possessing high activity against gram-negative bacteria. Special Considerations/Preparation Available as powder for injection in 2-g, 3-g, 4-g, and 40-g vials. Terminal Injection Site Incompatibility Amikacin, amiodarone, gentamicin, netilmicin, fluconazole, tobramycin, and vancomycin. Pharmacology Zosyn combines the extended-spectrum antibiotic piperacillin with the beta-lactamase inhibitor tazobactam in a 8:1 ratio. Piperacillin is primarily eliminated unchanged by renal mechanisms, whereas tazobactam undergoes significant hepatic metabolism. Reconstituted solution stable for 24 hours at room temperature, 48 hours refrigerated. These vials are intended for one-time, single-dose use, and the final concentration when diluted as directed by the manufacturer (5 mL per 1 g piperacillin) is not available. The entire contents of the single-dose vial should be withdrawn and further diluted to 10 to 40 mg/mL with a compatible solution prior to withdrawing the desired patient-specific dose. The desired dose should be further diluted to 10 to 40 mg/mL with a compatible solution prior to administration. Aminophylline, aztreonam, bumetanide, calcium gluconate, cefepime, cimetidine, clindamycin, dexamethasone, dopamine, enalaprilat, esmolol, fluconazole, furosemide, heparin, hydrocortisone succinate, linezolid, lorazepam, magnesium sulfate, metoclopramide, metronidazole, milrinone, morphine, potassium chloride, ranitidine, remifentanil, sodium bicarbonate, trimethoprim/sulfamethoxazole, and zidovudine. Terminal Injection Site Incompatibility Acyclovir, amikacin, amiodarone, amphotericin B, azithromycin, caspofungin, dobutamine, famotidine, ganciclovir, gentamicin, netilmicin, tobramycin, and vancomycin. Vaccine should appear as a homogeneous white suspension; do not use if it cannot be resuspended. Care should be taken to draw back on the plunger of the syringe before injection to be certain the needle is not in a blood vessel. Contraindications/Precautions Contraindicated in patients with a serious allergic reaction (eg, anaphylaxis) after a previous pneumococcal vaccine dose, or any diphtheria toxoid-containing vaccine. Adverse Effects Local injection site reactions (eg, erythema, induration, and tenderness) are common (greater than 20%) after each injection. Systemic reactions (eg, fever, irritability, decreased appetite, or decreased/increased sleep) are common (greater than 20%). Rare anaphylactic reactions (eg, hives, swelling of the mouth, hypotension, breathing difficulty, and shock) have been reported. Monitoring Observe injection site for erythema, induration (common), palpable nodule (uncommon), or sterile abscess (rare). Most recent updates available on the National Immunization Program website. Pharmacology 676 Micormedex NeoFax Essentials 2014 Sterile suspension of types 1, 2, and 3 poliovirus inactivated with formaldehyde. When giving multiple vaccines, use a separate syringe for each and give at separate sites. Care should be taken to draw back on the plunger of the syringe before injection to be certain the needle is not in a blood vessel [2]. Uses Immunoprophylaxis against poliomyelitis caused by poliovirus types 1, 2 and 3 in infants 6 weeks or older, children, and adults [3] [2]. Contraindications/Precautions Contraindicated in patients with anaphylaxis or shock within 24 hours after dose, or to any component of the vaccine which includes neomycin, streptomycin, polymyxin B, formaldehyde, and 2-phenoxyethanol. Pharmacology Sterile suspension of types 1, 2, and 3 poliovirus inactivated with formaldehyde. The vaccine produced using a microcarrier culture technique of monkey kidney cells has enhanced potency. Administration For Endotracheal Tube Instillation Using a 5-French end-hole Catheter Clear the trachea of secretions. Discard excess through catheter so only total dose to be given 680 Micormedex NeoFax Essentials 2014 remains in syringe [1]. For Endotracheal Tube Instillation Using the Second Lumen of a Dual Lumen Endotracheal Tube Slowly withdraw entire contents of vial into a plastic syringe through a large (greater than 20 gauge) needle. Each mL of surfactant contains 80 mg of total phospholipids (54 mg of phosphatidylcholine of which 30. Monitoring Monitor clinical and laboratory tests frequently for appropriate oxygen therapy and ventilatory support [1]. If settling occurs during storage, gently turn vial upside-down in order to uniformly suspend. Unopened vials that have 681 Micormedex NeoFax Essentials 2014 been warmed to room temperature one time may be refrigerated within 24 hours and stored for future use. Slowly withdraw entire contents of vial into a plastic syringe through a large (greater than 20 gauge) needle. Discard excess through catheter so only total dose to be given remains in syringe [1]. Keep infant in the neutral position and briefly disconnect the endotracheal tube from the ventilator and instill the first aliquot (1. Infant should be positioned so that either right or left side is dependent for the aliquot. Reposition the infant so that the other side is dependent and administer the remaining aliquot with the same procedure [1]. For Endotracheal Tube Instillation Using the Second Lumen of a Dual Lumen Endotracheal Tube 682 Micormedex NeoFax Essentials 2014 Slowly withdraw entire contents of vial into a plastic syringe through a large (greater than 20 gauge) needle. Keep the infant in a neutral position and administer as a single dose through the proximal end of the secondary lumen of the endotracheal tube. Curosurf is a modified porcine-derived minced lung extract containing phospholipids, neutral lipids, fatty acids, and surfactantassociated proteins B and C. Adverse Effects Transient episodes of reflux of bradycardia, hypotension, endotracheal tube blockage, and oxygen desaturation have been reported during administration [1]. Unopened vials that have been warmed to room temperature one time may be refrigerated within 24 hours and stored for future use. References Collaborative European Multicenter Study Group: Surfactant replacement therapy for severe neonatal respiratory distress syndrome: A international randomized clinical trial. Other signs of potassium toxicity include paresthesia of the extremities, weakness, and mental confusion [1] [2]. Hypokalemia in critically ill neonates is usually the result of diuretic (furosemide, thiazides) therapy or diarrhea. Special Considerations/Preparation Potassium chloride for injection is supplied as 2-mEq/mL solution. Various oral solutions are available, with concentrations ranging from 10 to 40 mEq per 15 mL. Title Potassium chloride Dose 685 Micormedex NeoFax Essentials 2014 Initial oral replacement therapy: 0. Maximum concentration: 40 mEq/L for peripheral, 80 mEq/L for central venous infusions. Alkalosis, as well as insulin infusions, will lower serum potassium concentrations by driving the ion intracellularly. Use with caution (if at all) in patients receiving potassium-sparing diuretics. Special Considerations/Preparation 686 Micormedex NeoFax Essentials 2014 Potassium chloride for injection is supplied as 2-mEq/mL solution. Other oral forms available include powder packets, tablets, and sustained-release capsules. Administration Intravenous/Intraosseous: Administer loading dose over 30 to 60 minutes at a concentration of 20 mg/mL. For continuous infusion, administer at a concentration of 2 to 4 mg/mL [1] [2] [3]. Contraindications/Precautions Contraindicated in patients with complete heart block and torsades de pointes [3]. Black Box Warning the use of procainamide hydrochloride as well as other antiarrhythmic agents should be reserved for patients with life-threatening ventricular arrhythmias. The rate of acetylation is primarily genetically determined in adults and children. Increasing frequency of toxicity associated with procainamide levels greater than 10 mcg/mL [3]. Special Considerations/Preparation 688 Micormedex NeoFax Essentials 2014 Available in 10-mL vials providing 100 mg/mL or 2-mL vials providing 500 mg/mL. Dilute initial bolus dose to a final concentration of 20 mg/mL prior to administration. Terminal Injection Site Compatibility Amiodarone, dobutamine, famotidine, flumazenil, heparin, hydrocortisone, lidocaine, netilmicin, ranitidine, remifentanil, and sodium nitroprusside. Acute treatment of ventricular tachycardia unresponsive to cardioversion and adenosine. Agranulocytosis, bone marrow depression, neutropenia, hypoplastic anemia, and thrombocytopenia in patients receiving procainamide hydrochloride have been reported (in adults), some of which were fatal. Renal function is a significant determinant of procainamide clearance [4] [3] [10]. Adverse Effects Severe hypotension with rapid infusion, bradycardia, A-V block, and ventricular fibrillation have been reported in adult patients. Special Considerations/Preparation Available in 10-mL vials providing 100 mg/mL or 2-mL vials providing 500 mg/mL. Maintenance infusion should be diluted to 2 to 4 mg/mL in compatible solution before administration [3]. Terminal Injection Site Compatibility 691 Micormedex NeoFax Essentials 2014 Amiodarone, dobutamine, famotidine, flumazenil, heparin, hydrocortisone, lidocaine, netilmicin, ranitidine, remifentanil, and sodium nitroprusside. Bouhouch R, El Houari T, Fellat I et al: Pharmacological therapy in children with nodal reentry tachycardia: when, how and how long to treat the affected patients.
Buy 100 mg cafergot fast delivery. Gout pain/Arthritis Gone is the Name of King Yeshua Jesus Christ.
References:
- http://www.bccancer.bc.ca/chemotherapy-protocols-site/Documents/Lymphoma-Myeloma/MYBORPRE_Protocol.pdf
- https://ec.europa.eu/health/ph_systems/docs/eunethta_report_en.pdf
- https://dev.org.es/research-center/buy-online-clonidine-cheap/
- http://jpp.krakow.pl/journal/archive/12_05_s6/pdf/45_12_05_s6_article.pdf
- http://www.med.umich.edu/pdf/gi/NAFLD_booklet5_22_17.pdf