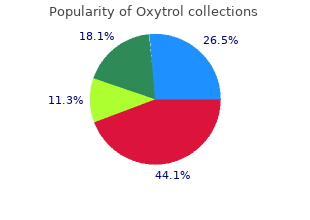
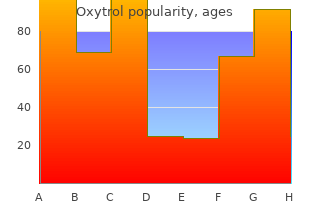
"Cheap oxytrol 2.5 mg with amex, symptoms nausea headache."
By: Cristina Gasparetto, MD
- Professor of Medicine
- Member of the Duke Cancer Institute

https://medicine.duke.edu/faculty/cristina-gasparetto-md
The same should be considered for family contacts of children in diapers attending centers where outbreaks occur and cases are recognized in 3 or more families treatment knee pain purchase oxytrol 5mg free shipping. In endemic areas new medicine buy 2.5 mg oxytrol otc, travellers should take only hot or bottled beverages and hot treatment trichomoniasis order oxytrol 5mg with amex, well-cooked food treatment zone guiseley order oxytrol 5mg with visa. Epidemic measures: 1) Determine mode of transmission (person-to-person or com mon vehicle) through epidemiological investigation; identify the population exposed medicine x protein powder discount 5 mg oxytrol free shipping. Specic outbreak control measures must be tailored to medicine kim leoni purchase oxytrol 5mg on line the characteristics of hepatitis A epide miology and of the existing hepatitis A immunization pro gram, if any, in the community. Immunization of older children who have not previously received vaccine should be accelerated in communities with ongoing programs of rou tine hepatitis A immunization for young children; target immunization should be undertaken for groups or areas (age groups, risk groups, census tracts) where local surveillance and epidemiological data show the highest rates. In outbreak settings such as day care, hospitals, institutions and schools, routine use of hepatitis A vaccine is not warranted. These immunization programs may reduce disease incidence only in the group(s) targeted. Disaster implications: Hepatitis A is a potential problem in large collections of people with overcrowding, inadequate san itation and water supplies; if cases occur, increased efforts should be exerted to improve sanitation and safety of water supplies. Mass administration of hepatitis A vaccine, which should be carefully planned, is not a substitute for environmental measures. In those with clinical illness, the onset is usually insidious, with anorexia, vague abdominal discomfort, nausea and vomiting, some times arthralgias and rash, often progressing to jaundice. Severity ranges from inapparent cases detectable only by liver function tests to fulminating, fatal cases of acute hepatic necrosis. Persons with chronic infection may or may not have a history of clinical hepatitis. About one-third have elevated amino transferases; biopsy ndings range from normal to chronic active hepatitis, with or without cirrhosis. HbsAg is present in serum during acute infections and persists in chronic infections. Most of these infections would be prevented by perinatal vaccination against hepatitis B of all newborns or infants. Serological evidence of previous infection may vary depending on age and socioeconomic class. Contaminated and inadequately sterilized syringes and needles have resulted in outbreaks of hepatitis B among patients; this has been a major mode of transmission worldwide. Chimpanzees are susceptible, but an animal reservoir in nature has not been recognized. Closely related hepadnavi ruses are found in woodchucks, ducks, ground squirrels and other animals such as snow leopards and German herons; none cause disease in humans. Sexual transmission from infected men to women is about 3 times more efficient than that from infected women to men. Anal intercourse, insertive or receptive, is associated with an increased risk of infection. Blood from experimentally inoculated volun teers has been shown to be infective weeks before the onset of rst symptoms and to remain infective through the acute clinical course of the disease. Disease is often milder and anicteric in children; in infants it is usually asymptomatic. Preventive measures: 1) Effective hepatitis B vaccines have been available since 1982. Immuni zation of successive infant cohorts produces a highly immune population and suffices to interrupt transmis sion. In mid-1999, it was announced that very small infants who receive multiple doses of vaccines containing thiomersal/thimerosal were at risk of receiving more than the recommended limits for mercury exposure as set out by industrialized guidelines. On the basis of a hypothetical risk of mercury exposure, reduction or elimination of thiomersal/thimerosal in vac cines as rapidly as possible was encouraged, although pharmacological and epidemiological data render it highly unlikely that such vaccines give rise to neurologi cal adverse effects. The greatest fall in incidence and prevalence of hepatitis B is in countries with high vaccine coverage at birth or in infancy. Vaccination of adolescents is also valuable as it protects against transmission through sexual contact or injection drug use. A sterile syringe and needle are essential for each individual receiving skin tests, parenteral inoculations or venepuncture. Discourage tattooing; enforce aseptic sanitary practices in tattoo par lours, including proper disposal of sharp or cutting tools. Notify blood banks of potential carriers so that future donations may be identied promptly. Control of patient, contacts and the immediate environment: 1) Report to local health authority: Official report obligatory in some countries; Class 2 (see Reporting). Studies show that alpha interferon is successful in arresting viral replication in about 25%�40% of treated patients. Lamivudine has fewer side-effects and is easier to administer, but has a modest efficacy rate, requires long-term treatment to maintain response, and is associated with a high rate of viral resistance, particularly when pro longed. Epidemic measures: When 2 or more cases occur in associa tion with some common exposure, search for additional cases. If a plasma derivative such as antihemophilic factor, brinogen, pooled plasma or thrombin is implicated, withdraw the lot from use and trace all recipients of the same lot in a search for additional cases. Disaster implications: Relaxation of sterilization precautions and emergency use of unscreened blood for transfusions may result in an increased number of cases. Identication�Onset is usually insidious, with anorexia, vague abdominal discomfort, nausea and vomiting; progression to jaundice less frequent than with hepatitis B. Although initial infection may be asymp tomatic (more than 90% of cases) or mild, a high percentage (50%�80%) develop a chronic infection. Of chronically infected persons, about half will eventually develop cirrhosis or cancer of the liver. Sexual and mother-to-child have been documented but appears far less efficient or frequent than the parenteral route. Chronic infection may persist for up to 20 years before the onset of cirrhosis or hepatoma. Period of communicability�From one or more weeks before onset of the rst symptoms; may persist in most persons indenitely. Routine virus inactiva tion of plasma-derived products, risk reduction counselling for persons uninfected but at high risk. For the treatment of chronic hepatitis C, highest response rates (40�80%) have been achieved with a combination therapy of ribavirin and slow-release interferons (�pegylated inter ferons�), making it the treatment of choice. However, these medications have signicant side-effects that require careful monitoring. International measures: Ensure adequate virus inactivation for all internationally traded biological products. In the former case the infection is usually self-limiting, in the latter it will usually progress to chronic hepatitis and delta hepatitis can be misdiagnosed as an exacerbation of chronic hepatitis B. Children may have a severe clinical course with usual progression to severe chronic hepatitis. Period of communicability�Blood is potentially infectious dur ing all phases of active delta hepatitis infection. Control of patient, contacts and the immediate environment, Epidemic measures, Disaster implications and International measures: See hepatitis B. Identication�Clinical course similar to that of hepatitis A; no evidence of a chronic form. The case-fatality rate is similar to that of hepatitis A except in pregnant women, where it may reach 20% among those infected during the third trimester of pregnancy. Diagnosis depends on clinical and epidemiological features and exclu sion of other causes of hepatitis, especially hepatitis A, by serological means. Outbreaks of hepatitis E and sporadic cases occur over a wide geographic area, primarily in countries with inadequate environmental sanitation. Out breaks often occur as waterborne epidemics, but sporadic cases and epidemics not clearly related to water have been reported. Outbreaks have also been reported from Algeria, Bangladesh, China, Cote d�Ivoire, Egypt, Ethiopia, Greece, India, Indone sia, the Islamic Republic of Iran, Jordan, the Libyan Arab Jamahiryia, Mexico, Myanmar, Nepal, Nigeria, Pakistan, southern areas of the Russian Federation, Somalia, eastern Sudan and the Gambia. Natural infections have been described in pigs, chicken and cattle, particularly in highly endemic areas. Mode of transmission�Primarily by the fecal-oral route; fecally contaminated drinking-water is the most commonly documented vehicle of transmission. Person-to-person transmission probably also occurs through the fecal-oral route, although secondary household cases are uncommon during outbreaks. Recent studies suggest that hepatitis E may in fact be a zoonotic infection with coincident areas of high human infection. Incubation period�The range is 15 to 64 days; the mean incuba tion period has varied from 26 to 42 days in various epidemics. Women in the third trimester of pregnancy are especially susceptible to fulminant disease. The occurrence of major epidemics among young adults in regions where other enteric viruses are highly endemic and most of the population acquires infection in infancy remains unexplained. Preventive measures: Provide educational programs to stress sanitary disposal of feces and careful handwashing after defeca tion and before handling food; follow basic measures to prevent fecal-oral transmission, as listed under Typhoid fever, 9A. Control of patient, contacts and the immediate environment: 1), 2) and 3) Report to local health authority, Isolation and Concurrent disinfection: See hepatitis A. Epidemic measures: Determine mode of transmission through epidemiological investigation; investigate water supply and iden tify populations at increased risk of infection; special efforts to improve sanitary and hygienic practices in order to eliminate fecal contamination of foods and water. Disaster implications: A potential problem where there is mass crowding and inadequate sanitation and water supplies. If cases occur, increased effort should be exerted to improve sanitation and the safety of water supplies. Identication�Herpes simplex is a viral infection characterized by a localized primary lesion, latency and a tendency to localized recurrence. Reactivation of latent infection commonly results in herpes labialis (fever blisters, cold sores) manifested, usually on the face or lips, by supercial clear vesicles on an erythematous base that crust and heal within days. Reactivation is precipitated by various forms of trauma, fever, physiological changes or intercurrent disease, and may also involve other body tissues; it occurs in the presence of circulating antibodies, which are seldom elevated by reactivation. Severe and extensive spread of infection may occur in those who are immunodecient or immunosuppressed. Fever, headache, leukocytosis, meningeal irritation, drowsiness, confu sion, stupor, coma and focal neurological signs may occur and are frequently referable to one or the other temporal region. The condition may be confused with other intracranial lesions including brain abscess and tuberculous meningitis. In women, the principal sites of primary disease are the cervix and the vulva; recurrent disease generally involves the vulva, perineal skin, legs and buttocks. In men, lesions appear on the glans penis or prepuce, and in the anus and rectum of those engaging in anal sex. Neonatal infections can be divided into 3 clinical presentations: dissem inated infections involving the liver, encephalitides and infections limited to the skin, eyes or mouth. Only excretion at the time of delivery is dangerous to the newborn, with the rare exception of intrauterine infections. Primary infection in the mother raises the risk of infection from 3% to over 30%, presumably because maternal immunity confers a degree of protection. A 4-fold titre rise in paired sera in various serological tests conrms the diagnosis of primary infection; the presence of herpes-specic IgM is suggestive but not conclusive evidence of primary infection. Infectious agent�Herpes simplex virus in the virus family Herpes viridae, subfamily Alphaherpesvirinae. The prevalence is greater (up to 60%) in lower socioeconomic groups and persons with multiple sexual partners. Both types 1 and 2 may be transmitted to various sites by oral-genital, oral-anal or anal-genital contact. In recurrent lesions, infectivity is shorter than after primary infection, and usually the virus cannot be recovered after 5 days. Preventive measures: 1) Health education and personal hygiene directed toward minimizing the transfer of infectious material. The risk of fatal neonatal infection after a recurrent infection is much lower (3%�5%), and caesarean section advisable only when active lesions are present at delivery. Control of patient, contacts and the immediate environment: 1) Report to local health authority: Official case report in adults not ordinarily justiable, Class 5; neonatal infections report able in some areas, Class 3 (see Reporting). Patients with herpetic lesions should have no contact with newborns, children with eczema or burns, or immunodecient patients. Corticosteroids should never be used for ocular involvement unless administered by an experienced ophthal mologist. Acyclovir used orally, intravenously or topically has been shown to reduce shedding of virus, diminish pain and accelerate healing time in primary genital and recurrent herpes, rectal herpes and herpetic whitlow. The oral prepa ration is most convenient to use and may benet patients with extensive recurrent infections. However, mutant strains of herpes virus resistant to acyclovir have been reported. Valacyclovir and famciclovir are recently licensed congeners of acyclovir that have equivalent efficacy. This causes an ascending encephalomyelitis seen in veterinarians, laboratory workers and others in close contact with eastern Hemisphere monkeys or monkey cell cultures. After an incubation of 3 days to 3 weeks, there is acute febrile onset with headache, often local vesicular lesions, lympho cytic pleocytosis and variable neurological patterns, ending in death in over 70% of cases, 1 day to 3 weeks after onset of symptoms. Occasional recoveries have been associated with considerable residual disability; a few cases, treated with acyclovir, have recovered completely. During periods of stress (shipping and handling), they have high rates of viral shedding. Human illness, rare but highly fatal, is acquired through the bite of apparently normal monkeys, or exposure of naked skin or mucous membrane to infected saliva or monkey cell cultures.
Jha June 3 treatment action campaign purchase oxytrol 2.5 mg fast delivery, 2014; 82: e188-e193 194 A 33-year-old woman with severe postpartum occipital headaches 221 An 87-year-old woman with left-sided numbness N medications 2016 buy oxytrol american express. This book would not have been possible without the encouragement of Patty Baskin withdrawal symptoms oxytrol 5mg without prescription, Executive Editor medicine in motion cheap 2.5mg oxytrol otc, and the leadership of Dr medicine 91360 purchase 5 mg oxytrol overnight delivery. Bob Gross medicine 3604 effective 5 mg oxytrol, Editor-in-Chief, both of whom have always been tremendous supporters of the Resident & Fellow Section. Finally, and in particular, we acknowledge Kathy Pieper, Managing Editor of Neurology, for her dedication, passion, and commitment to excellence in this project, as in so many others. The quality of the content is superb, submissions are plentiful, and our staff of young editors is enthusiastic and talented. These case discussions are the stuff by which we all learned neurology, and are here collected to educate trainees across the country. This effort also serves as a reminder of the educational mission of the section, which is now giving back to our community beyond its usual publications. Elkind, of extensive �book knowledge��neuroanatomy, that is at the core of clinical neurology. To see the clinical effects of precise lesions lished in the Clinical Reasoning section describing firsthand, to hear the stories of patients suffering from diverse diagnoses, challenging clinical quandaries, neurologic disease, and to discuss these findings with and daunting management dilemmas. Most were one�s clinical teachers at the bedside: these are the written by residents and fellows, supervised by fac experiences that transform students of neurology into ulty, and are thus geared toward those learning clini clinical neurologists. Many of these fascinating the process of clinical reasoning is learned through cases and the accompanying discussions, however, practice: trying to localize the lesion that explains a pa are likely to be as informative to experienced neurol tient�s symptoms and signs, attempting to reconcile ogists as to trainees. For this anthology we have com disparate elements of the history and examination, piled cases that span the major cardinal presentations judging when to obtain and how to interpret neuro of neurologic disease. Each section begins with a brief diagnostic tests, conferring on complex cases with one�s introduction to the clinical approach for a particular peers and mentors, and seeing the evolution of neuro realm of neurology, but leaves the detailed discussions logic disease and how it may be modified by treatment. Yet such experiences shared between colleagues or We hope that our readers will enjoy the opportu between teachers and students are rarely recorded nity to learn from this collection, case by case. Berkowitz has received speaker honoraria from Stevens Institute for case reports that capture the art and science of of Technology and AudioDigest, and receives publishing royalties for Clin ical Pathophysiology Made Ridiculously Simple, MedMaster, 2007andThe clinical neurology. Declarative memory as complex cognitive functions including attention, relies upon the integrity of the Papez circuit in memory, language, visuospatial processing, and the mesial temporal lobes and diencephalon, emotional processing. These are the quintessential including entorhinal cortex, the hippocampus, functions that make us human. In the context of the fornix, the mammillary bodies, the mammil neurologic illness it is possible to witness the extent lothalamic tract, the anterior nucleus of the thal to which the elements of cognition can become frac amus, and the cingulate cortex. Diseases that tured and separable; dysfunction in individual cog affect these structures produce anterograde amne nitive domains helps us to understand their sia, with impaired ability to recall newly encoded fundamental nature. A careful examination of rior temporal lobe, the arcuate fasciculus, and the a patient�s mental state can therefore yield enor Broca area in the inferior frontal lobe. This network mous information about the localization and differ is typically represented in the left hemisphere, but ential diagnosis of lesions affecting the cerebral there may be bilateral or right hemispheric repre hemispheres. Homologous areas in � Arousal relies upon connections from the ascending the right hemisphere contribute to the generation reticular activating system, which originates in the and processing of music as well as prosody of lan rostral brainstem and projects to both thalami and guage. The evaluation of sions in the rostral brainstem or in both hemi language function includes an assessment of flu spheres can impair arousal, placing a patient on a ency, naming, repetition, comprehension, reading, spectrum of states of altered consciousness that in and writing. Lesions in the language networks pro cludes drowsiness, somnolence, obtundation, duce aphasia, which may be characterized as recep a minimally responsive vegetative state, and coma. To evaluate atten � Visuospatial processing relies upon distributed net tional mechanisms, one can observe the patient�s works that compose the �dorsal stream, � which in ability to answer directed questions and avoid dis cludes parietal areas specialized for processing tractions. Lesions that dis assessing digit span, having the patient spell a word rupt right parietal areas and their networks may backwards, or having the patient continue specific produce the clinical syndrome of hemispatial patterns. Higher-order visual processing also relies lateral prefrontal cortex demonstrate impaired on a �ventral stream, � which includes inferior tem attention and working memory. Lesions of the poral areas specialized for processing visual features medial frontal lobes can produce akinetic mutism, of an object, a face, or a scene. Lesions of the orbi formed by the limbic system of the brain, which tofrontal cortex produce disinhibited behaviors that includes the cingulate cortex, amygdala, thalamus, may transgress accepted social norms. These regions contribute to � Memory can be divided into declarative memory consciously experienced emotions but also have (which encompasses episodic memory for auto strong connections with functions unconsciously biographical events and recognition memory for carried out by the autonomic nervous system. Perrier Memory Center of an academic hospital for progres activities autonomously. His past medical history in tation progressed until he ultimately got lost in the C. There was no family history of any psychiat he began making sexually inappropriate comments that ric or neurologic disorders. Address correspondence and the patient�s symptoms began 3 years prior to pre the neuropsychological evaluation upon ad reprint requests to Dr. Karl sentation with memory loss and word-finding difficul mission revealed a severe amnestic syndrome, dif Mondon, Centre Memoire de Ressources et de Recherche, ties. Six months later, his wife observed a progressive ficulties in naming and verbal comprehension, Hopital Bretonneau, 2 Bd loss of interest in his previous hobbies and increasing visuospatial impairment, a cognitive and behav Tonnelle, 37044 Tours, Cedex, France apathy. Twelve months after symptom onset, the pa ioral prefrontal syndrome, and multimodal visual karl. At the same time, his wife observed a personal neurologic examination was normal. First, potentially curable causes of dementia When pyramidal, cerebellar, or choreiform movements should be excluded. Motor im pugilistica), or inflammatory (multiple sclerosis) le pairment or a concurrent movement disorder suggests sions. Laboratory tests assess the most frequent endo subcortical causes of dementia such as Parkinson disease crine and metabolic disorders (thyroid, parathyroid, dementia, progressive supranuclear palsy, and cortico B12, thiamine, folate and niacin deficiencies, hypo basal degeneration. Finally, global (Alzheimer disease) glycemia, hepatic encephalopathy, renal failure). Laboratory tests of with a widespread increase in theta activity, predom the adrenal and pituitary functions could be per inately in the temporal regions. Metabolic studies can assess for leukodystro bilateral temporal lobe atrophy, markedly more se phies, encephalopathies, and porphyria. If sleep vere on the right side (figure), while the other cortical apnea is suspected, polysomnography can be under regions, including the frontal lobes, were normal. If imaging suggests normal pressure hydro There were no white matter abnormalities. Question for consideration: If the evaluation remains inconclusive, degenerative etiologies should be considered. International Classification of Diseases and Health Related Problems, 10th Revision. Geneva: World Health Organi dromes, which can be divided into 3 groups: 1) zation; 1992. Frequency and 7 clinical characteristics of early-onset dementia in consecu tia lacking distinctive histopathology. Dement Geriatr Cogn the right temporal variant is a fourth and rare Disord 2007; 24:42�47. The accurate diagnosis of early-onset demen long time, prosopagnosia was considered the main tia. Lancet Neurol 2007; 6:734� and identifying the faces of familiar persons due to 8 746. Frontotemporal Thus, the right temporal variant of frontotemporal lobar degeneration: a consensus on clinical diagnostic cri lobar degeneration can be considered to be the right teria. Frontotemporal dementia and related disor Recently, investigators delineated the cognitive pro ders: deciphering the enigma. Brain 2009; 132(Pt symptom is topographic disorientation (getting lost) in 5):1287�1298. Questions for consideration: On the day prior to presentation, the patient began having memory difficulties and was noted by her 1. What is the differential diagnosis for subacute Correspondence to husband to have completely forgotten many events memory disturbances and confusion in this Dr. Infectious workup was notable for a rapid confusion or exposure to psychoactive medications influenza swab that was positive for influenza A. Finally, transient Questions for consideration: global amnesia is a consideration, but is a diagnosis of exclusion. What is the differential diagnosis of subacute intracranial imaging to assess for mass lesion, altered mental status and seizures in association stroke, or hemorrhage. Reflexes were brisk, measuring 3/4 in all abnormalities; thus, the seizures should be viewed as 4 extremities, and the patient had positive Hoffman symptomatic of another pathologic process until signs, flexor plantar response on the right, and equiv proven otherwise. How do you interpret the results of lumbar the patient was treated with acyclovir and levetira puncture On enza, and Cryptococcus as well as testing for enterovi follow-up 8 months later, the patient was fully ambu ruses or arboviruses depending on the season. Repeat lumbar puncture in the mesial temporal lobes and thalami consistent showed total protein of 794 mg/dL, glucose of with necrotizing encephalitis. Additional extensive 84 mg/dL, with 4 leukocytes and 19 erythrocytes workup for infectious encephalitis was negative. Chest X-ray demonstrated a association with symmetric hemorrhagic brain left lower lobe opacity, and the patient was treated lesions. McCray cared for the patient presented, wrote the text, and Eur J Pediatr 2011; 170:1007�1015. Jenelle Acute hemorrhagic leukoencephalopathy associated with Jindal cared for the patient and helped in discussion of the manuscript. Elkind, previous residences, and forgot her children�s tentive and abulic with sparse but fluent speech. She recalled 2 of 3 words at 5 minutes, but had no mem presented to the obstetrical service fully dilated af ory for recent events, including her delivery. She ter 2 days of leaking vaginal fluid, and delivered a could not describe cocktail ingredients, despite work Address correspondence and healthy baby girl. A few hours later, she did not ing as a bartender, but correctly recited old addresses. Grinspan, Division of Pediatric Neurology, Harkness neurology service for evaluation. Pavilion, 5th Floor, 180 Fort She had had a febrile seizure at age 4, and several Strength was full. She had 2 healthy Questions for consideration: children, 1 abruption at 23 weeks, and 1 elective 1. Subacute processes, such as de onset encephalopathy with memory loss and abulia, myelinating diseases and paraneoplastic processes, as well as long tract signs. Focal insults to Serum chemistries were normal except for low total structures responsible for memory or attention, such protein (5. Lumbar puncture re the differential diagnosis includes emergent vealed a protein of 121 mg/dL, normal glucose, 3 white peripartum conditions, such as dural sinus throm 3 3 blood cells/mm, and 23 red blood cells/mm. Urine bosis, metastatic choriocarcinoma, and postpar tum angiopathy, a form of reversible cerebral toxicology was positive for marijuana. Neurology 73 October 13, 2009 e7513 agulation, endocrine, cardiac, lipid, and immunologic caliber changes in the distal branches of both middle studies were unrevealing. Subtle memory problems had be hypointense on T1-weighted imaging and some gun 1 month prior. There were multi Questions for consideration: ple lesions in the corpus callosum, many with a rim of T2 hyperintensity around a center of T1 hypoin 1. What further testing would help distinguish among these worsens over hours to days, and lasts days to weeks, diagnoses Digital tance of the history in an encephalopathic patient and subtraction angiography found generalized small cal the utility of a broad differential diagnosis. Bedside under 100 m in the cochlea, retina, and brain (rather dilated funduscopic examination revealed bilateral than muscle and skin, as in dermatomyositis). The current literature only describes about 100 pa Muscle biopsy and additional serum tests to look for tients with Susac syndrome, but the disease is underap evidence of endothelial damage were obtained. Women dothelial antibody tests were weakly positive, and factor outnumber men 3:1. Months to years may separate the initial symp cells, and may rise if they are damaged. We diagnosed Susac syndrome, or retinocochleo often migrainous, frequently precedes the onset of en cerebral vasculopathy, based on the pathognomonic cephalopathy, and progresses to confusion, memory loss, behavioral changes, dysarthria, and mutism. Only after an unrevealing evaluation for matter lesions in the cerebral hemispheres. Also of show restricted diffusion, suggesting they represent note, initial bedside funduscopic examination found small infarcts. The character tum, she demonstrated right visual field deficits, brisk istic callosal lesions in Susac syndrome are frequently reflexes, and clonus at both ankles, right more than left. However, their Seven months postpartum, she continues to take myco central location, �snowball� appearance on T2 phenolate mofetil, and is slowly tapering prednisone. She fatigues easily, but manages household chores size of the affected arterioles is below the resolution of and childcare on her own. Tullman has received research support from Acorda Ther sionally monocular amaurosis fugax. Post partum cerebral angiopathy: reversible vasoconstriction as Only 7 pregnancies in 6 patients with Susac syn sessed by transcranial Doppler ultrasounds. Susac�s nant women with inflammatory myopathy often syndrome: 1975�2005 microangiopathy/autoimmune en respond to steroids alone, and may flare postpartum. Retinocochleoce tion, and as many as 1/3 have relapse of encephalop rebral vasculopathy. Mycophenolate mofetil was added after weighted imaging and apparent diffusion coefficient val a week, as she had not significantly improved, and the dis ues.
Terlipressin and albumina vs [222] Keller F medicine gif order discount oxytrol, Heinze H treatment upper respiratory infection 5mg oxytrol mastercard, Jochimson F medications over the counter cheap oxytrol 5 mg without prescription, Passfall J symptoms 6 days post iui discount oxytrol 5mg otc, Schuppan D medications xanax buy 2.5 mg oxytrol, Buttner P medications just like thorazine oxytrol 2.5 mg low cost. Risk albumina in patients with cirrhosis and hepatorenal syndrome: a random factors and outcome of 107 patients with decompensated liver disease and ized study. Therapy with vasoconstrictor drugs in cirrhosis: the hepatorenal syndrome maintained on hemodialysis. Trans [216] Angeli P, Volpin R, Gerunda G, Craighero R, Roner P, Merenda R, et al. Effects of noradrenalin and albumin in patients with type I Effects of treatment of hepatorenal syndrome before transplantation on hepatorenal syndrome: a pilot study. J Hepatol 2004; 40: [219] Akriviadis E, Bortla R, Briggs W, Han S, Reynolds T, Shakil O. Pentoxifylline improves short-term survival in severe acute alcoholic Journal of Hepatology 2010 vol. The symptoms include fever, petechial or maculopapular Corresponding Author: Amar Taksande rash and arthralgia or arthrits afectng multple joints mainly in adults. The tme of greatest risk of transmission from mother to fetus appears during birth if mother amar. Pediatrics, Jawaharlal Nehru Medical College, Sawangi Meghe, Wardha, Keywords: Chikungunya virus, Fever, Neonate Maharashtra 442102 Introducton Case Report Chikungunya is a relatvely rare form of viral fever caused by A 6-day old female baby presented to us with history of fever an alphavirus that is spread by mosquito bites from the Aedes since 3 day. Lumsden in 1955, following an outbreak to 24-year old, 2nd gravida mother at 38-weeks of gestaton. There on the Makonde Plateau, along the border between Tanganyika were no history of pregnancy induced hypertension, diabetes or and Mozambique, in 1952. Symptoms appear between 4 and 7 antenatal problems in the mother except for high grade fever days afer the patent has been biten by the infected mosquito. The A high fever and headache occur, with signifcant pains in the mother was conservatvely treated for fever at home. There are cried immediately afer birth and was put on the breast feeds not many reports of clinical features of confrmed chikungunya within one hour. Neonates present at 3-5 days of life, baby brought to the hospital for high grade, contnuous type life with fever, excessive crying, dermatological manifestatons fever along with irritability. On admission baby was excessively like maculopapular rash, nasal blotchy erythema, freckle like irritable and contnuously crying. Anterior pigmentaton over centrofacial area, vesiculobullous lesions, fontanelle was not bulging. Her weighed 25600gm, length 52cm apnea, shock, disseminated intravascular coagulaton. Capillary reflling tme was < of greatest risk of transmission from mother to fetus appears 3second. Cardiovascular, respiratory and neurological examinaton was Viral chikungunya perinatally transmited leads to encephalits in normal. Baby was discharged on 10th day of delivery, sixteen newborns were symptomatc in the neonatal of life. The tme of greatest risk of transmission from mother to fetus appears during birth if mother acquired the disease days Discussion before delivery. It is transmited to humans by mosquitoes 16 weeks and suggest the virus played a direct role in fetal deaths. Most ofen chikungunya been derived from a Makonde word meaning �that which bends is a self-limitng febrile illness and responded to conservatve or up�. Chikungunya was frst neurocognitve functons of infants infected by maternal-fetal described in Tanzania, Africa in 1952. They found infected children India in 1963, when along with dengue, it caused very extensive exhibit poorer neurocognitve skills than uninfected peers, as epidemic in Calcuta, Madras, and other areas. Chikungunya evidenced by lower global developmental quotent scores and outbreaks occurred at irregular interval along the east coast diminished specifc neurocognitve skills. It can cause a debilitatng illness and the poorest neurocognitve outcome and prostraton. The neurocognitve outcome of infected manifestatons are relatvely rare and as a rule shock is not children is poor and must be monitored throughout childhood to observed in chikungunya virus infecton. Neurological complicatons such as conclusion, this case report shows that viral chikungunya can be meningoencephalits have been reported in patents during the transmited from mother to babies and clinical presentaton is frst Indian outbreak as well as the recent French Reunion islands similar to that of septcemia or meningits. Lancet 368: et al (2006) Chikungunya infection in pregnancy: Evidence for 186-187. The breathing difculties associated with this disease can be very distressing and frighten Pertussis, commonly known as whooping cough, is ing for the patient and his or her family. In addition, adults with pertussis How long does it take to show signs of pertussis infection have been shown to be a frequent source of after being exposed The incubation period of pertussis is commonly 7 to 10 What are possible complications from pertussis Younger patients have a greater chance of complica What are the symptoms of pertussis The most common complication is secondary bacterial infection, Pertussis disease can be divided into three stages: which is the cause of most pertussis-related deaths. Catarrhal stage: can last 1�2 weeks and includes a Pneumonia occurs in one out of 20 cases; this percent runny nose, sneezing, low-grade fever, and a mild age is higher for infants younger than age 6 months. Infants are also more likely to sufer from such neuro Paroxysmal stage: usually lasts 1�6 weeks, but can per logic complications as seizures and encephalopathy, sist for up to 10 weeks. The characteristic symptom is a probably due to the reduction of oxygen supply to the burst, or paroxysm, of numerous, rapid coughs. Other less serious complications include ear end of the cough paroxysm, the patient can sufer from infection, loss of appetite, and dehydration. Although the cough usually disap pears after 2�3 weeks, paroxysms may recur whenever How do I know if my child has pertussis The disease is usually milder in adolescents and characteristic history and physical examination. A labo adults, consisting of a persistent cough similar to that ratory test may be done, which involves taking a speci found in other upper respiratory infections. Pertussis can be a very serious disease, especially for How long is a person with pertussis contagious Infants (6 months of age and younger) are People with pertussis are most infectious during the the children most likely to die from this disease. Rates catarrhal period and during the frst two weeks after of hospitalization and complications increase with onset of the cough (approximately 21 days). Before a vaccine against pertussis was available, per tussis (whooping cough) was a major cause of child How are vaccines made that prevent diphtheria, hood illness and death in the United States. With the introduction of a vaccine in the late these vaccines are made by chemically treating the 1940s, the number of reported pertussis cases in the diphtheria, tetanus, and pertussis toxins to render U. They are known as �inactivated� vaccines because they do not contain live Since the 1980s, the number of cases of pertussis has bacteria and cannot replicate themselves, which is why increased, especially among babies younger than 6 multiple doses are needed to produce immunity. In recent years, several states have reported a signifcant increase in cases, with out What�s the diference between all the vaccines breaks of pertussis reaching epidemic levels in some containing diphtheria and tetanus toxoids and states. The frst inactivated toxin, or toxoid, against diphtheria was developed around 1921, but it was not widely used � Tdap: Tetanus and diphtheria toxoids with acellular until the 1930s. In 1924, the frst tetanus toxoid (inac pertussis vaccine; adolescents and adults. Pregnant tivated toxin) was produced and was used successfully women should receive Tdap during each pregnancy. The frst pertussis vaccine was developed in the and adults ages 7 years and older. In tion in the anterolateral thigh muscle (for infants and 1991, concerns about safety led to the development young toddlers) or in the deltoid muscle (for older chil of more purifed (acellular) pertussis vaccines that are dren and adults). In 2005, two new vaccine products were licensed for All children, beginning at age 2 months, and adults use in adolescents and adults that combine the tetanus need protection against these three diseases�diphthe and diphtheria toxoids with acellular pertussis (Tdap) ria, tetanus, and pertussis (whooping cough). These vaccines are the frst acellular pertussis booster doses are also needed throughout life. What side efects have been reported with these At least one of the doses, preferably the frst, should be vaccines Local reactions, such as redness and swelling at the Because immunity to diphtheria and tetanus wanes injection site, and soreness and tenderness where the with time, boosters of Td or Tdap are needed every ten shot was given, as well as mild systemic reactions such years. When adolescents and adults are scheduled for Side efects following Td or Tdap in older children and their routine tetanus and diphtheria booster, adults include redness and swelling at the injection site (following Td) and generalized body aches, and tired should they get vaccinated with Td or Tdap Older children and adults who Immunization experts recommend that a dose of received more than the recommended doses of Td/ Tdap be given to all adolescents at age 11�12 years as Tdap vaccine can experience increased local reactions, a booster during the routine adolescent immuniza such as painful swelling of the arm. This is due to the tion visit if the adolescent has fnished the childhood high levels of tetanus antibody in their blood. If the levels of diphtheria antitoxin and 100% will have protec catch-up dose is given at age 10, it can count as the tive levels of tetanus antitoxin in their blood. Then, subsequent booster doses of mates of acellular pertussis vaccine efcacy range from Td or Tdap should be given every ten years. Pregnant 80% to 85%, but protection declines as the time since teens and women should receive Tdap during each the dose increases. Adolescents and adults who have recently received Td vaccine can be given Tdap without any wait Can a pregnant woman receive Tdap vaccine All pregnant women should receive Tdap during If someone experiences a deep or puncture wound, or each pregnancy, preferably early in the time period a wound contaminated with dirt, an additional booster between 27 and 36 weeks� gestation. Recent studies dose of either Td or Tdap may be given if the last dose show that vaccination during pregnancy reduces a was more than fve years ago. Because infants are not adequately protected Tdap since their 7th birthday, give Tdap. If a new mother hasn�t been vac continued on the next page Immunization Action Coalition � Saint Paul, Minnesota � 651-647-9009 � A precaution means that a person would usu ally not receive the vaccine but there may be occasions Who should not receive these vaccines Precautions include: Guillain-Barre syndrome vaccine should not receive another dose of the same (a rare type of neurological condition) within 6 weeks vaccine. Im not sure how much of this detail is o Causes required (probably little, from the length of the block), but it was in Robbins, so its in here. See the Thrombosis end of this section, page 12, for tables of the really � Atherosclerosis (most common) important stuff. No physical findings on the brain With recurrent events, the memory loss will get longer and longer, typical sports injury Contusion Bruising of brain from impact with the cranial vault; crests of frontal and temporal lobes most susceptible. Coup (site of injury) and contracoup (diamterically opposite) develop when the head is mobile at the time of impact. Compression of brain stem is fatal Everything we�ve talked about since congenital malformations goes hand in hand, so is included here in a review. It is called o Neuromyelitis Optica = Asians, Bilateral optic neuritis, relentlessly destructive a plaque. Xiong did not differentiate between the o Fatal in many patients; some live without permanent complications two types, though Robbins o Macro = Grayish discoloration of white matter; multiple global lesions that did. W ellcircum scribed dem yelinated plaques � active, Com m on (1:1000) Dem yelinating V ision loss (optic neuritis). Elevated Dem yelinating w ith potential recovery and potential fatality thinning or loss. Occurs in kids and adolescents Encephalom yelitis Central Pontine M etabolic Spastic Q uadraparesis Bilateral, sym m etrical dem yelination of w hite Seen in alcoholics, hyperosm olar states, or M yelinolysis Dem yelinating M ental changes, m ay produce the �lockedin� m atter in the basis ponti electrolyte im balances. Severe Strict V egans and pernicious anem ia; requires Degeneration Dem yelinating follow ed by spastic paralysis. Irreversible cases m ay involve entire cord circum ference decades to deplete B12 stores. M etachrom atic Inborn Progressive peripheral neuropathy, blindness, Diffuse loss of m yelin in w hite m atter, Autosom al recessive disease caused by Leukodystrophy Dysm yelinating retardation, childhood onset, adult dem entia accum ulation of sulfatide in oligodendrocytes arylsulfatase deficiency giving a �m arbled� appearance to the parenchym a Adreno InBorn Adrenal Insufficiency begins in childhood Diffuse m yelin loss w ith lipidladen histiocytes. Xlinked m utation for the peroxisom e protein leukodystrophy Dysm yelinating Neurologic m anifestations (behavior, vision, W hite m atter atrophy. By the time hydrocephalus ex vacuo is noticeable, the patient is deep into their dementia, too deep to be helped. Lesions here result in atrophy, areflexia, and weakness leading to paralysis o Upper Motor Neurons are found along the length of the spinal cord and into the brain. Weirnicke�s may appear, giving way Korsakoff is memory loss and to chronic, irreversible Korsakoff confabulation B12 Deficiency None, this is a Over decades, B12 stores get Common in strict vegans and in deficiency of diet depleted, neurons/myelin die pernicious anemia. Huge gene, tear themselves apart Progressive muscle weakness; in a lots of opportunity for breakage wheelchair by 10, dead by 20. Becker�s Xlinked recessive mutation Because it dystrophin is not gone, Normal Life Span, patients have a slower, Muscular (but not loss) of the dystrophin it is simply a milder form of the more variable progression. Often have thymic growths Lambert Paraneoplsatic syndrome of Antibodies against the presynaptic Proximal Muscle Weakness with Eaton small cell carcinoma of lung Calcium Channels of peripheral autonomic dysfunction. Weakness is worst muscle, limiting amount of in the morning but improves with activity neurotransmitter released but not with cholinesterase inhibitors Acing the Test: Duchenne is a worse form then Becker�s of the same disease; a mutation in dystrophin. LambertEaton gets better with use, no change with drugs, and affects proximal muscles 37 Owl Club Review Sheets. It is the largest systematic scientific effort in history to quantify levels and trends of health loss due to diseases, injuries, and risk factors. The higher points on the chart indicate that declines in mortality 0 rates were faster in those age groups between 1990 and 2010. Males aged 30-34 Age group years saw the smallest decrease in mortality rate (12%). For Cardio & circulatory diseases example, musculoskeletal Cancer disorders include low back 100, 000 Other communicable pain and neck pain.
Air movement for rooms with dashes and nonpatient areas may vary as necessary to medications not to take when pregnant buy oxytrol 5 mg visa satisfy the requirements of those spaces new medicine generic oxytrol 2.5mg line. Additional adjustments may be needed when space is unused or unoccupied and air systems are deenergized or reduced treatment of gout order oxytrol 5 mg line. Last update: July 2019 230 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) 3 symptoms viral infection buy oxytrol online. Areas not indicated as having continuous directional control may have ventilation systems shut down when space is unoccupied and ventilation is not otherwise needed symptoms 7dpiui oxytrol 2.5mg generic. Air from areas with contamination and/or odor problems shall be exhausted to medicine lux generic oxytrol 5 mg overnight delivery the outside and not recirculated to other areas. Note that individual circumstances may require special consideration for air exhaust to outside. Gravity type heating or cooling units such as radiators or convectors shall not be used in special care areas. Where temperature ranges are indicated, the systems shall be capable of maintaining the rooms at any point within the range. A single figure indicates a heating or cooling capacity of at least the indicated temperature. This is usually applicable where residents may be undressed and require a warmer environment. Nothing in these guidelines shall be construed as precluding the use of temperatures lower than those noted when the residents� comfort and medical conditions make lower temperatures desirable. The number of air changes may be reduced or varied to any extent required for odor control when the space is not in use. Last update: July 2019 231 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) Table B. Filter efficiencies for central ventilation and air conditioning systems in general hospitals* Number of filter Filter bed no. Filter efficiencies for central ventilation and air conditioning systems in outpatient facilities* Number of filter Filter bed no. Laboratories 1 80 n/a Administrative, bulk storage, soiled holding areas, 1 30 n/a food preparation areas, and laundries Note: this table is Table 9. Filter efficiencies for central ventilation and air conditioning systems in nursing facilities Minimum number Filter bed no. Filter efficiencies for central ventilation and air conditioning systems in psychiatric hospitals Minimum number Filter bed no. Last update: July 2019 232 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) Appendix C. These adherent organisms can initiate and develop biofilms, which are comprised of cells embedded in a matrix of extracellularly produced polymers and associated abiotic particles. In the health-care facility environment, biofilms may be found in the potable water supply piping, hot water tanks, air conditioning cooling towers, or in sinks, sink traps, aerators, or shower heads. Biofilms, especially in water systems, are not present as a continuous slime or film, but are more often scanty and heterogeneous in nature. Favorable conditions for biofilm formation are present if these structures and equipment are not cleaned for extended periods of time. Although most of these organisms will not normally pose a problem for healthy individuals, certain biofilm bacteria. Although the association of biofilms and medical devices provides a plausible explanation for a variety of health-care associated infections, it is not clear how the presence of biofilms in the water system may influence the rates of health-care� associated waterborne infection. Research has shown that biofilm-associated organisms are more resistant to antibiotics and disinfectants than are planktonic organisms, either because the cells are protected by the polymer matrix, or because they are physiologically different. Though chlorine in its various forms is a proven disinfectant, it has been shown to be less effective against biofilm bacteria. Routine sampling of health-care facility water systems for biofilms is not warranted. If an epidemiologic investigation points to the water supply system as a possible source of infection, then water sampling for biofilm organisms should be considered so that prevention and control strategies can be developed. Strategies to remediate biofilms in a water system would include flushing the system piping, hot water tank, dead legs, and those areas of the facility�s water system subject to low or intermittent flow. The general strategy for evaluating water system biofilm depends on a comparision of the bacteriological quality of the incoming municipal water and that of water sampled from within facility�s distribution system. Heterotrophic plate counts and coliform counts, both of which are routinely run by the municipal water utility, will at least provide in indication of the potential for biofilm formation. A direct correlation between heterotrophic plate count and biofilm levels has been demonstrated. The water supplied to the facility should also contain <1 coliform bacteria/100 mL. Coliform bacteria are organisms whose presence in the distribution system could indicate fecal contamination. It has been shown that coliform bacteria can colonize biofilms within drinking water systems. Intermittant contamination of a water system with these organisms could lead to colonization of the system. Water samples can be collected from throughout the health-care facility system, including both hot and cold water sources; samples should be cultured by standard methods. If biofilms are detected in the facility water system and determined by an epidemiologic and environmental investigation to be a reservoir for health-care associated pathogens, the municipal water supplier could be contacted with a request to provide higher chlorine residuals in the distribution system, or the health-care facility could consider installing a supplemental chlorination system. Samples are suspended by vortexing with sterile glass beads and plated onto a nonselective medium. In the case of an outbreak, it would be advisable to isolate organisms from these plates to determine whether the suspect organisms are present in the biofilm or water samples and compare them to the organisms isolated from patient specimens. Therefore, when the spread plate method is used, a pipette must be used to place 0. Several studies, however, have shown Last update: July 2019 234 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) that the use of nutrient-poor media, such as R2A, results in an increased recovery of bacteria from water. Extending the culturing time up to 168 hours, or 7 days and using incubation temperatures of 73. It should be recognized, however, that these culturing conditions may underestimate the bacterial burden in the water and fail to identify the presence of some organisms. Additionally, the recommended method will not detect fungi and yeast, which have been shown to contaminate water used for hemodialysis applications. Because endotoxins differ in their activity on a mass basis, their activity is referred to a standard Escherichia coli endotoxin. Water Sampling Strategies and Culture Techniques for Detecting Legionellae Legionella spp. Scheduled microbiologic monitoring for legionellae remains controversial because the presence of legionellae is not necessarily evidence of a potential for causing disease. Examination of water samples is the most efficient microbiologic method for identifying sources of legionellae and is an integral part of an epidemiologic investigation into health-care associated Legionnaires Last update: July 2019 235 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) disease. One environmental sampling protocol that addresses sampling site selection in hospitals might serve as a prototype for sampling in other institutions. The bacteria are rarely found in municipal water supplies and tend to colonize plumbing systems and point-of-use devices. To colonize, legionellae usually require a temperature range of 77�F�108�F (25�C�42. Therefore, air-conditioning equipment condensate, which frequently evaporates, is not a likely source. When culturing faucet aerators and shower heads, swabs of surface areas should be collected first; water samples are collected after aerators or shower heads are removed from their pipes. If the swabs and water samples must be transported back to a laboratory for processing, immersing individual swabs in sample water minimizes drying during transit. Place swabs and water samples in insulated coolers to protect specimens from temperature extremes. Procedures for collecting and processing environmental specimens for Legionella spp. Collect culture swabs of internal surfaces of faucets, aerators, and shower heads in a sterile, screw-top container. Submerge each swab in 5�10 mL of sample water taken from the same device from which the sample was obtained. Transport samples and process in a laboratory proficient at culturing water specimens for Legionella spp. Last update: July 2019 236 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) 4. Provide protective equipment to workers who perform the disinfection, to prevent their exposure to chemicals used for disinfection and aerosolized water containing Legionella spp. Shut off the automated blowdown controller, if present, and set the system controller to manual. Add fast-release, chlorine-containing disinfectant in pellet, granular, or liquid form, and follow safety instructions on the product label. The dispersant is best added by first dissolving it in water and adding the solution to a turbulent zone in the water system. Automatic-dishwasher compounds are examples of low or nonfoaming, silicate-based dispersants. After adding disinfectant and dispersant, continue circulating the water through the system. Because the biocidal effect of chlorine is reduced at a higher pH, adjust the pH to 7. Municipal water and sewerage authorities should be contacted regarding local regulations. If necessary, the drain-off may be dechlorinated by dissipation or chemical neutralization with sodium bisulfite. Last update: July 2019 237 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) G. Refill the system with water and repeat the procedure outline in steps 2�7 in I-B above. Circulate the water for 1 hour, then open the blowdown valve and flush the entire system until the water is free of turbidity. In the United Kingdom, where maintenance of water temperatures at 122�F (50�C) in hospitals has been mandated, installation of blending or mixing valves at or near taps to reduce the water temperature to 109. Increasing the flow rate from the hot-water circulation system may help lessen the likelihood of water stagnation and cooling. This requires the placement of flow-adjusted, continuous injectors of chlorine throughout the water distribution system. Adverse effects of continuous chlorination can include accelerated corrosion of plumbing (resulting in system leaks) and production of potentially carcinogenic trihalomethanes. Insects and Microorganisms Format Change [February 2016]: the format of this section was changed to improve readability and accessibility. Microorganisms isolated from arthropods in health-care settings Cockroaches Microorganism category Microorganisms References Gram-negative bacteria Acinetobacter spp. Information Resources the following sources of information may be helpful to the reader. Some of these are available at no charge, while others are available for purchase from the publisher. Similar information may be found at Sampling and Characterization of Bioaerosols. These documents may be purchased from: American Society of Heating, Refrigerating, and Air-Conditioning Engineers, Inc. Similar information may be found at Managing Water Infiltration into Buildings. The plan discusses infection control issues both for home-based care and hospital-based patient management. Animals in Health-Care Facilities � Service animal information with respect to the Americans with Disabilities Act. This is the Internet address on their Internet web site that will link to any state for information about medical waste rules and regulations at the state level: [This link is no longer active: Last update: July 2019 240 of 241 Guidelines for Environmental Infection Control in Health-Care Facilities (2003) Appendix F. Areas of Future Research Air � Standardize the methodology and interpretation of microbiologic air sampling. Water � Evaluate new methods of water treatment, both in the facility and at the water utility. Environmental Services � Evaluate the innate resistance of microorganisms to the action of chemical germicides, and determine what, if any, linkage there may be between antibiotic resistance and resistance to disinfectants. Laundry and Bedding � Evaluate the microbial inactivation capabilities of new laundry detergents, bleach substitutes, other laundry additives, and new laundry technologies. Animals in Health-Care Facilities � Conduct surveillance to monitor incidence of infections among patients in facilities that use animal programs, and conduct investigations to determine new infection control strategies to prevent these infections. Regulated Medical Waste � Determine the efficiency of current medical waste treatment technologies to inactivate emerging pathogens that may be present in medical waste. Johnson, Ruth Gilbert, and Mike Sharland, tibacterial drugs prescribed for skin infections, and used all on behalf of improving Children�s Antibiotic oral preparations containing ucloxacillin prescribed for Prescribing Group skin conditions as a proxy measure of unresolved S. We calculated age�sex adjusted annual for skin conditions for children <18 years of age in England consulting and prescribing rates by totaling the number of increased 19%, from 128. We then directly stan period, hospital admissions for Staphylococcus aureus in dardized these rates by using the age�sex distribution for fections rose 49% from 53. Therefore, its use provides a proxy marker rates per 100, 000 resident population for children <18 years of S. Flucloxacillin pre of age for each calendar year from January 1, 1997, through scribing in children has increased over the past 15 years December 31, 2006, for conditions commonly caused by S. Rates We examined the incidence of local complications of were calculated as the total number of admissions per year S.
Cheap oxytrol 2.5mg without a prescription. Hot toddy | soothes sore throat wards off cold and flu symptoms.
References:
- https://dev.org.es/research-center/purchase-online-frumil-no-rx/
- https://dev.org.es/research-center/buy-online-clonidine-cheap/
- http://5.imimg.com/data5/EQ/LX/XO/GLADMIN-59766/imtus-cancer-injection.pdf
- https://apps.who.int/iris/bitstream/handle/10665/325771/WHO-MVP-EMP-IAU-2019.06-eng.pdf?sequence=1&isAllowed=y
- https://www.hamiltonhealthsciences.ca/wp-content/uploads/2019/08/NAFLD-trh.pdf